PART 425 - MEDICARE SHARED SAVINGS PROGRAM
Source:
76 FR 67973, Nov. 2, 2011, unless otherwise noted.
Subpart A - General Provisions
§ 425.10 Basis and scope.
(a) Basis. This part implements section 1899 of the Act by establishing a shared savings program that promotes accountability for a patient population, coordinates items and services under Medicare parts A and B, and encourages investment in infrastructure and redesigned care processes for high quality and efficient services. The regulations under this part must not be construed to affect the payment, coverage, program integrity, and other requirements that apply to providers and suppliers under FFS Medicare, except as permitted under section 1899(f) of the Act.
(b) Scope. This part sets forth the following:
(1) The eligibility requirements for an ACO to participate in the Medicare Shared Savings Program (Shared Savings Program).
(2) Application procedures and provisions of the participation agreement.
(3) Program requirements and beneficiary protections.
(4) The method for assigning Medicare fee-for-service beneficiaries to ACOs.
(5) Quality performance standards, reporting requirements, and data sharing.
(6) Payment criteria and methodologies (one-sided model and two-sided models).
(7) Compliance monitoring and sanctions for noncompliance.
(8) Reconsideration review process.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32833, June 9, 2015]
§ 425.20 Definitions.
As used in this part, unless otherwise indicated -
Accountable care organization (ACO) means a legal entity that is recognized and authorized under applicable State, Federal, or Tribal law, is identified by a Taxpayer Identification Number (TIN), and is formed by one or more ACO participants(s) that is(are) defined at § 425.102(a) and may also include any other ACO participants described at § 425.102(b).
ACO participant means an entity identified by a Medicare-enrolled billing TIN through which one or more ACO providers/suppliers bill Medicare, that alone or together with one or more other ACO participants compose an ACO, and that is included on the list of ACO participants that is required under § 425.118.
ACO participant agreement means the written agreement (as required at § 425.116) between the ACO and ACO participant in which the ACO participant agrees to participate in, and comply with, the requirements of the Shared Savings Program.
ACO professional means an individual who is Medicare-enrolled and bills for items and services furnished to Medicare fee-for-service beneficiaries under a Medicare billing number assigned to the TIN of an ACO participant in accordance with applicable Medicare regulations and who is either of the following:
(1) A physician legally authorized to practice medicine and surgery by the State in which he or she performs such function or action.
(2) A practitioner who is one of the following:
(i) A physician assistant (as defined at § 410.74(a)(2) of this chapter).
(ii) A nurse practitioner (as defined at § 410.75(b) of this chapter).
(iii) A clinical nurse specialist (as defined at § 410.76(b) of this chapter).
ACO provider/supplier means an individual or entity that meets all of the following:
(1) Is a -
(i) Provider (as defined at § 400.202 of this chapter); or
(ii) Supplier (as defined at § 400.202 of this chapter).
(2) Is enrolled in Medicare.
(3) Bills for items and services furnished to Medicare fee-for-service beneficiaries during the agreement period under a Medicare billing number assigned to the TIN of an ACO participant in accordance with applicable Medicare regulations.
(4) Is included on the list of ACO providers/suppliers that is required under § 425.118.
ACO's regional service area means all counties where one or more beneficiaries assigned to the ACO reside.
Agreement period means the term of the participation agreement.
Antitrust Agency means the Department of Justice or Federal Trade Commission.
Assignable beneficiary means a Medicare fee-for-service beneficiary who receives at least one primary care service with a date of service during a specified 12-month assignment window from a Medicare-enrolled physician who is a primary care physician or who has one of the specialty designations included in § 425.402(c).
Assignment means the operational process by which CMS determines whether a beneficiary has chosen to receive a sufficient level of the requisite primary care services from ACO professionals so that the ACO may be appropriately designated as exercising basic responsibility for that beneficiary's care during a given benchmark or performance year.
Assignment window means the 12-month period used to assign beneficiaries to an ACO.
At-risk beneficiary means, but is not limited to, a beneficiary who -
(1) Has a high risk score on the CMS-HCC risk adjustment model;
(2) Is considered high cost due to having two or more hospitalizations or emergency room visits each year;
(3) Is dually eligible for Medicare and Medicaid;
(4) Has a high utilization pattern;
(5) Has one or more chronic conditions.
(6) Has had a recent diagnosis that is expected to result in increased cost.
(7) Is entitled to Medicaid because of disability; or
(8) Is diagnosed with a mental health or substance abuse disorder.
BY stands for benchmark year.
Certified Electronic Health Record Technology (CEHRT) has the same meaning given this term under § 414.1305 of this chapter.
Continuously assigned beneficiary means a beneficiary assigned to the ACO in the current performance year who was either assigned to or received a primary care service from any of the ACO participants during the assignment window for the most recent prior benchmark or performance year.
Covered professional services has the same meaning given these terms under section 1848(k)(3)(A) of the Act.
Critical access hospital (CAH) has the same meaning given this term under § 400.202 of this chapter.
Eligible clinician has the same meaning given this term under § 414.1305 of this chapter.
Eligible professional has the meanings given this term under section 1848(k)(3)(B) of the Act.
Experienced with performance-based risk Medicare ACO initiatives means an ACO that CMS determines meets the criteria in either paragraph (1) or (2) of this definition.
(1) The ACO is the same legal entity as a current or previous ACO that is participating in, or has participated in, a performance-based risk Medicare ACO initiative as defined under this section, or that deferred its entry into a second Shared Savings Program agreement period under a two-sided model under § 425.200(e).
(2) Forty percent or more of the ACO's ACO participants participated in a performance-based risk Medicare ACO initiative, as defined under this section, or in an ACO that deferred its entry into a second Shared Savings Program agreement period under a two-sided model under § 425.200(e), in any of the 5 most recent performance years prior to the agreement start date.
Federally qualified health center (FQHC) has the same meaning given to this term under § 405.2401(b) of this chapter.
High revenue ACO means an ACO whose total Medicare Parts A and B fee-for-service revenue of its ACO participants based on revenue for the most recent calendar year for which 12 months of data are available, is at least 35 percent of the total Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries based on expenditures for the most recent calendar year for which 12 months of data are available.
Hospital means a hospital as defined in section 1886(d)(1)(B) of the Act.
Inexperienced with performance-based risk Medicare ACO initiatives means an ACO that CMS determines meets all of the following:
(1) The ACO is a legal entity that has not participated in any performance-based risk Medicare ACO initiative as defined under this section, and has not deferred its entry into a second Shared Savings Program agreement period under a two-sided model under § 425.200(e).
(2) Less than 40 percent of the ACO's ACO participants participated in a performance-based risk Medicare ACO initiative, as defined under this section, or in an ACO that deferred its entry into a second Shared Savings Program agreement period under a two-sided model under § 425.200(e), in each of the 5 most recent performance years prior to the agreement start date.
Low revenue ACO means an ACO whose total Medicare Parts A and B fee-for-service revenue of its ACO participants based on revenue for the most recent calendar year for which 12 months of data are available, is less than 35 percent of the total Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries based on expenditures for the most recent calendar year for which 12 months of data are available.
Marketing materials and activities include, but are not limited to, general audience materials such as brochures, advertisements, outreach events, letters to beneficiaries, Web pages, data sharing opt out letters, mailings, social media, or other activities conducted by or on behalf of the ACO, or by ACO participants, or ACO providers/suppliers participating in the ACO, when used to educate, solicit, notify, or contact Medicare beneficiaries or providers and suppliers regarding the Shared Savings Program. The following beneficiary communications are not marketing materials and activities: Certain informational materials customized or limited to a subset of beneficiaries; materials that do not include information about the ACO, its ACO participants, or its ACO providers/suppliers; materials that cover beneficiary-specific billing and claims issues or other specific individual health related issues; educational information on specific medical conditions (for example, flu shot reminders), written referrals for health care items and services, and materials or activities that do not constitute “marketing” under 45 CFR 164.501 and 164.508(a)(3)(i).
Medicare fee-for-service beneficiary means an individual who is -
(1) Enrolled in the original Medicare fee-for-service program under both parts A and B; and
(2) Not enrolled in any of the following:
(i) A MA plan under part C.
(ii) An eligible organization under section 1876 of the Act.
(iii) A PACE program under section 1894 of the Act.
Newly assigned beneficiary means a beneficiary that is assigned to the ACO in the current performance year who was neither assigned to nor received a primary care service from any of the ACO participants during the assignment window for the most recent prior benchmark or performance year.
One-sided model means a model under which the ACO may share savings with the Medicare program, if it meets the requirements for doing so, but is not liable for sharing any losses incurred under subpart G of this part.
Participation agreement means the written agreement required under § 425.208(a) between the ACO and CMS that, along with the regulations in this part, govern the ACO's participation in the Shared Savings Program.
Performance-based risk Medicare ACO initiative means, for purposes of this part, an initiative implemented by CMS that requires an ACO to participate under a two-sided model during its agreement period, including the following options and initiatives:
(1) Participation options within the Shared Savings Program as follows:
(i) BASIC track (Levels A through E).
(ii) ENHANCED track.
(iii) Track 2.
(2) The Innovation Center ACO models under which an ACO accepts risk for shared losses as follows:
(i) Pioneer ACO Model.
(ii) Next Generation ACO Model.
(iii) Comprehensive ESRD Care Model two-sided risk tracks.
(iv) Track 1+ Model.
(3) Other initiatives involving two-sided risk as may be specified by CMS.
Performance year means the 12-month period beginning on January 1 of each year during the agreement period, unless otherwise specified in § 425.200(c) or noted in the participation agreement.
Physician means a doctor of medicine or osteopathy (as defined in section 1861(r)(1) of the Act).
Physician Quality Reporting System (PQRS) means the quality reporting system established under section 1848(k) of the Act.
Primary care physician means:
(1) For performance years 2012 through 2015, a physician included in an attestation by the ACO as provided under § 425.404 for services furnished in an FQHC or RHC, or a physician who has a primary care specialty designation of internal medicine, general practice, family practice, or geriatric medicine;
(2) For performance years 2016 through 2018, a physician included in an attestation by the ACO as provided under § 425.404 for services furnished in an FQHC or RHC, or a physician who has a primary care specialty designation of internal medicine, general practice, family practice, geriatric medicine, or pediatric medicine; and
(3) For performance year 2019 and subsequent years, a physician who has a primary care specialty designation of internal medicine, general practice, family practice, geriatric medicine, or pediatric medicine.
Primary care services means the set of services identified by the HCPCS and revenue center codes designated under § 425.400(c).
Quality measures means the measures defined by the Secretary, under section 1899 of the Act, to assess the quality of care furnished by an ACO, such as measures of clinical processes and outcomes, patient and, where practicable, caregiver experience of care and utilization.
Re-entering ACO means an ACO that does not meet the definition of a renewing ACO and meets either of the following conditions:
(1) Is the same legal entity as an ACO, as defined in this section, that previously participated in the program and is applying to participate in the program after a break in participation, because it is either -
(i) An ACO whose participation agreement expired without having been renewed; or
(2) Is a new legal entity that has never participated in the Shared Savings Program and is applying to participate in the program and more than 50 percent of its ACO participants were included on the ACO participant list under § 425.118, of the same ACO in any of the 5 most recent performance years prior to the agreement start date.
Renewing ACO means an ACO that continues its participation in the program for a consecutive agreement period, without a break in participation, because it is either -
(1) An ACO whose participation agreement expired and that immediately enters a new agreement period to continue its participation in the program; or
(2) An ACO that terminated its current participation agreement under § 425.220 and immediately enters a new agreement period to continue its participation in the program.
Reporting period, for purposes of subpart F of this part, means the calendar year from January 1 to December 31.
Rural health center (RHC) has the same meaning given to this term under § 405.2401(b).
Taxpayer Identification Number (TIN) means a Federal taxpayer identification number or employer identification number as defined by the IRS in 26 CFR 301.6109-1.
Two-sided model means a model under which the ACO may share savings with the Medicare program, if it meets the requirements for doing so, and is also liable for sharing any losses incurred under subpart G of this part.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32833, June 9, 2015; 80 FR 71385, Nov. 16, 2015; 81 FR 38013, June 10, 2016; 82 FR 53368, Nov. 15, 2017; 83 FR 60092, Nov. 23, 2018; 83 FR 68062, Dec. 31, 2018]
Subpart B - Shared Savings Program Eligibility Requirements
§ 425.100 General.
(a) Under the Shared Savings Program, ACO participants may work together to manage and coordinate care for Medicare fee-for-service beneficiaries through an ACO that meets the criteria specified in this part. The ACO must become accountable for the quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to the ACO.
(b) An ACO is eligible to receive payments for shared savings under subpart G of this part if all of the following conditions are met:
(1) The ACO meets or exceeds the applicable minimum savings rate established under § 425.604, § 425.605, § 425.606, § 425.609, or § 425.610.
(2) The ACO meets the minimum quality performance standards established under § 425.500 (for performance years or a performance period beginning on or before January 1, 2020), or under the quality performance standard established under § 425.512 (for performance years beginning on or after January 1, 2021).
(3) The ACO otherwise maintains its eligibility to participate in the Shared Savings Program under this part.
(c) ACOs that operate under a two-sided model and meet or exceed a minimum loss rate established under § 425.605, § 425.606, § 425.609 or § 425.610 must share losses with the Medicare program under subpart G of the part.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32834, June 9, 2015; 83 FR 60092, Nov. 23, 2018; 83 FR 68083, Dec. 31, 2018; 85 FR 85038, Dec. 28, 2020]
§ 425.102 Eligible providers and suppliers.
(a) The following ACO participants or combinations of ACO participants are eligible to form an ACO that may apply to participate in the Shared Savings Program:
(1) ACO professionals in group practice arrangements.
(2) Networks of individual practices of ACO professionals.
(3) Partnerships or joint venture arrangements between hospitals and ACO professionals.
(4) Hospitals employing ACO professionals.
(5) CAHs that bill under Method II (as described in § 413.70(b)(3) of this chapter).
(6) RHCs.
(7) FQHCs.
(8) Teaching hospitals that have elected under § 415.160 of this subchapter to receive payment on a reasonable cost basis for the direct medical and surgical services of their physicians.
(b) Other ACO participants that are not identified in paragraph (a) of this section are eligible to participate through an ACO formed by one or more of the ACO participants identified in paragraph (a) of this section.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 71386, Nov. 16, 2015]
§ 425.104 Legal entity.
(a) An ACO must be a legal entity, formed under applicable State, Federal, or Tribal law, and authorized to conduct business in each State in which it operates for purposes of the following:
(1) Receiving and distributing shared savings.
(2) Repaying shared losses or other monies determined to be owed to CMS.
(3) Establishing, reporting, and ensuring provider compliance with health care quality criteria, including quality performance standards.
(4) Fulfilling other ACO functions identified in this part.
(b) An ACO formed by two or more ACO participants, each of which is identified by a unique TIN, must be a legal entity separate from any of its ACO participants.
(c) An ACO formed by a single ACO participant may use its existing legal entity and governing body, provided it satisfies the other requirements in §§ 425.104 and 425.106.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32834, June 9, 2015]
§ 425.106 Shared governance.
(a) General rule.
(1) An ACO must maintain an identifiable governing body with ultimate authority to execute the functions of an ACO as defined under this part, including but not limited to, the processes defined under § 425.112 to promote evidence-based medicine and patient engagement, to report on quality and cost measures, and to coordinate care.
(2) The governing body of the ACO must satisfy all of the following criteria:
(i) Be the same as the governing body of the legal entity that is the ACO.
(ii) Be separate and unique to the ACO and must not be the same as the governing body of any ACO participant, except as provided in § 425.104(c).
(iii) Satisfy all other requirements of this section.
(b) Responsibilities of the governing body and its members.
(1) The governing body must have responsibility for oversight and strategic direction of the ACO, holding ACO management accountable for the ACO's activities as described in this part.
(2) The governing body must have a transparent governing process.
(3) The governing body members must have a fiduciary duty to the ACO, including the duty of loyalty, and must act consistent with that fiduciary duty.
(c) Composition and control of the governing body.
(1) The ACO must—
(i) Establish a mechanism for shared governance among the ACO participants or combinations of ACO participants (as identified in § 425.102(a)) that formed the ACO; and
(ii) Provide for meaningful participation in the composition and control of the ACO's governing body for ACO participants or their designated representatives.
(2) The ACO governing body must include a Medicare beneficiary who—
(i) Is served by the ACO;
(ii) Is not an ACO provider/supplier;
(iii) Does not have a conflict of interest with the ACO; and
(iv) Does not have an immediate family member who has a conflict of interest with the ACO.
(3) At least 75 percent control of the ACO's governing body must be held by ACO participants.
(4) The governing body members may serve in a similar or complementary manner for an ACO participant.
(5) In cases in which the composition of the ACO's governing body does not meet the requirements of paragraphs (c)(2) and (c)(3) of this section, the ACO must describe why it seeks to differ from these requirements and how the ACO will involve ACO participants in innovative ways in ACO governance or provide meaningful representation in ACO governance by Medicare beneficiaries.
(d) Conflict of interest. The ACO governing body must have a conflict of interest policy that applies to members of the governing body. The conflict of interest policy must—
(1) Require each member of the governing body to disclose relevant financial interests; and
(2) Provide a procedure to determine whether a conflict of interest exists and set forth a process to address any conflicts that arise.
(3) The conflict of interest policy must address remedial action for members of the governing body that fail to comply with the policy.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32835, June 9, 2015]
§ 425.108 Leadership and management.
(a) An ACO must have a leadership and management structure that includes clinical and administrative systems that align with and support the goals of the Shared Savings Program and the aims of better care for individuals, better health for populations, and lower growth in expenditures.
(b) The ACO's operations must be managed by an executive, officer, manager, general partner, or similar party whose appointment and removal are under the control of the ACO's governing body and whose leadership team has demonstrated the ability to influence or direct clinical practice to improve efficiency processes and outcomes.
(c) Clinical management and oversight must be managed by a senior-level medical director. The medical director must be all of the following:
(1) A board-certified physician.
(2) Licensed in a State in which the ACO operates.
(3) Physically present on a regular basis at any clinic, office or other location of the ACO, an ACO participant, or an ACO provider/supplier.
(d) Each ACO participant and each ACO provider/supplier must demonstrate a meaningful commitment to the mission of the ACO to ensure the ACO's likely success.
(1) Meaningful commitment may include, for example, a sufficient financial or human investment (for example, time and effort) in the ongoing operations of the ACO such that the potential loss or recoupment of the investment is likely to motivate the ACO participant and ACO provider/supplier to achieve the ACO's mission under the Shared Savings Program.
(2) A meaningful commitment can be shown when an ACO participant or ACO provider/supplier agrees to comply with and implement the ACO's processes required by § 425.112 and is held accountable for meeting the ACO's performance standards for each required process.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32835, June 9, 2015]
§ 425.110 Number of ACO professionals and beneficiaries.
(a)
(1) The ACO must include primary care ACO professionals that are sufficient for the number of Medicare fee-for-service beneficiaries assigned to the ACO under subpart E of this part. The ACO must have at least 5,000 assigned beneficiaries.
(2) CMS deems an ACO to have initially satisfied the requirement to have at least 5,000 assigned beneficiaries as specified in paragraph (a)(1) of this section if 5,000 or more beneficiaries are historically assigned to the ACO participants in each of the 3 benchmark years, as calculated using the assignment methodology set forth in subpart E of this part. In the case of the third benchmark year, CMS uses the most recent data available to estimate the number of assigned beneficiaries.
(b) If at any time during the performance year, an ACO's assigned population falls below 5,000, the ACO may be subject to the actions described in §§ 425.216 and 425.218.
(1) While under a CAP, the ACO remains eligible for shared savings and liable for shared losses.
(2) If the ACO's assigned population is not at least 5,000 by the end of the performance year specified by CMS in its request for a CAP, CMS terminates the participation agreement and the ACO is not eligible to share in savings for that performance year.
(3) In determining financial performance for an ACO with fewer than 5,000 assigned beneficiaries, the MSR/MLR is calculated as follows:
(i) For ACOs with a variable MSR and MLR (if applicable), the MSR and MLR (if applicable) are set at a level consistent with the number of assigned beneficiaries.
(ii) For performance years starting before July 1, 2019, for ACOs with a fixed MSR/MLR, the MSR/MLR remains fixed at the level consistent with the choice of MSR and MLR that the ACO made at the start of the agreement period.
(iii) For performance years starting on July 1, 2019 and in subsequent years, for ACOs that selected a fixed MSR/MLR at the start of the agreement period or prior to entering a two-sided model during their agreement period, the MSR/MLR is calculated as follows:
(A) The MSR/MLR is set at a level based on the number of beneficiaries assigned to the ACO.
(1) The MSR is the same as the MSR that would apply in a one-sided model under § 425.604(b) (for Track 2 ACOs) or § 425.605(b)(1) (for BASIC track and ENHANCED track ACOs) and is based on the number of assigned beneficiaries.
(2) The MLR is equal to the negative MSR.
(B) The MSR and MLR revert to the fixed level previously selected by the ACO for any subsequent performance year in the agreement period in which the ACO's assigned beneficiary population is 5,000 or more.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32835, June 9, 2015; 81 FR 80559, Nov. 15, 2016; 83 FR 68063, Dec. 31, 2018]
§ 425.112 Required processes and patient-centeredness criteria.
(a) General.
(1) An ACO must—
(i) Promote evidence-based medicine and beneficiary engagement, internally report on quality and cost metrics, and coordinate care;
(ii) Adopt a focus on patient centeredness that is promoted by the governing body and integrated into practice by leadership and management working with the organization's health care teams; and
(iii) Have defined processes to fulfill these requirements.
(2) An ACO must have a qualified healthcare professional responsible for the ACO's quality assurance and improvement program, which must include the defined processes included in paragraphs (b)(1) through (4) of this section.
(3) For each process specified in paragraphs (b)(1) through (4) of this section, the ACO must—
(i) Require ACO participants and ACO providers/suppliers to comply with and implement each process (and subelement thereof), including the remedial processes and penalties (including the potential for expulsion) applicable to ACO participants and ACO providers/suppliers for failure to comply with and implement the required process; and
(ii) Employ its internal assessments of cost and quality of care to improve continuously the ACO's care practices.
(b) Required processes. The ACO must define, establish, implement, evaluate, and periodically update processes to accomplish the following:
(1) Promote evidence-based medicine. These processes must cover diagnoses with significant potential for the ACO to achieve quality improvements taking into account the circumstances of individual beneficiaries.
(2) Promote patient engagement. These processes must address the following areas:
(i) Compliance with patient experience of care survey requirements in § 425.500 or § 425.510, as applicable.
(ii) Compliance with beneficiary representative requirements in § 425.106.
(iii) A process for evaluating the health needs of the ACO's population, including consideration of diversity in its patient populations, and a plan to address the needs of its population.
(A) In its plan to address the needs of its population, the ACO must describe how it intends to partner with community stakeholders to improve the health of its population.
(B) An ACO that has a stakeholder organization serving on its governing body will be deemed to have satisfied the requirement to partner with community stakeholders.
(iv) Communication of clinical knowledge/evidence-based medicine to beneficiaries in a way that is understandable to them.
(v) Beneficiary engagement and shared decision-making that takes into account the beneficiaries' unique needs, preferences, values, and priorities;
(vi) Written standards in place for beneficiary access and communication, and a process in place for beneficiaries to access their medical record.
(3) Develop an infrastructure for its ACO participants and ACO providers/suppliers to internally report on quality and cost metrics that enables the ACO to monitor, provide feedback, and evaluate its ACO participants and ACO provider(s)/supplier(s) performance and to use these results to improve care over time.
(4) Coordinate care across and among primary care physicians, specialists, and acute and post-acute providers and suppliers. The ACO must—
(i) Define its methods and processes established to coordinate care throughout an episode of care and during its transitions, such as discharge from a hospital or transfer of care from a primary care physician to a specialist (both inside and outside the ACO); and
(ii) Have a written plan to:
(A) Implement an individualized care program that promotes improved outcomes for, at a minimum, the ACO's high-risk and multiple chronic condition patients.
(B) Identify additional target populations that would benefit from individualized care plans. Individualized care plans must take into account the community resources available to the individual.
(C) Encourage and promote use of enabling technologies for improving care coordination for beneficiaries. Enabling technologies may include one or more of the following:
(1) Electronic health records and other health IT tools.
(2) Telehealth services, including remote patient monitoring.
(3) Electronic exchange of health information.
(4) Other electronic tools to engage beneficiaries in their care.
(D) Partner with long-term and post-acute care providers, both inside and outside the ACO, to improve care coordination for its assigned beneficiaries.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32835, June 9, 2015; 82 FR 53368, Nov. 15, 2017; 85 FR 85038, Dec. 28, 2020]
§ 425.114 Participation in other shared savings initiatives.
(a) ACOs may not participate in the Shared Savings Program if they include an ACO participant that participates in the independence at home medical practice pilot program under section 1866E of the Act, a model tested or expanded under section 1115A of the Act that involves shared savings, or any other Medicare initiative that involves shared savings.
(b) CMS will review and deny an ACO's application if any ACO participants are participating in another Medicare initiative that involves shared savings payments.
(c) CMS will determine an appropriate method to ensure no duplication in payments for beneficiaries assigned to other shared savings programs or initiatives, including initiatives involving dually eligible beneficiaries, when such other shared savings programs have an assignment methodology that is different from the Shared Savings Program.
§ 425.116 Agreements with ACO participants and ACO providers/suppliers.
(a) ACO participant agreements. For performance year 2017 and subsequent performance years, the ACO must have an ACO participant agreement with each ACO participant that complies with the following criteria:
(1) The only parties to the agreement are the ACO and the ACO participant.
(2) The agreement must be signed on behalf of the ACO and the ACO participant by individuals who are authorized to bind the ACO and the ACO participant, respectively.
(3) The agreement must expressly require the ACO participant to agree, and to ensure that each ACO provider/supplier billing through the TIN of the ACO participant agrees, to participate in the Shared Savings Program and to comply with the requirements of the Shared Savings Program and all other applicable laws and regulations (including, but not limited to, those specified at § 425.208(b)).
(4) The agreement must set forth the ACO participant's rights and obligations in, and representation by, the ACO, including without limitation, the quality reporting requirements set forth in subpart F of this part, the beneficiary notification requirements set forth at § 425.312, and how participation in the Shared Savings Program affects the ability of the ACO participant and its ACO providers/suppliers to participate in other Medicare demonstration projects or programs that involve shared savings.
(5) The agreement must describe how the opportunity to receive shared savings or other financial arrangements will encourage the ACO participant to adhere to the quality assurance and improvement program and evidence-based medicine guidelines established by the ACO.
(6) The agreement must require the ACO participant to update its enrollment information, including the addition and deletion of ACO professionals and ACO providers/suppliers billing through the TIN of the ACO participant, on a timely basis in accordance with Medicare program requirements and to notify the ACO of any such changes within 30 days after the change.
(7) The agreement must permit the ACO to take remedial action against the ACO participant, and must require the ACO participant to take remedial action against its ACO providers/suppliers, including imposition of a corrective action plan, denial of incentive payments, and termination of the ACO participant agreement, to address noncompliance with the requirements of the Shared Savings Program and other program integrity issues, including those identified by CMS.
(8) The agreement must be for a term of at least 1 performance year and must articulate potential consequences for early termination from the ACO.
(9) The agreement must require completion of a close-out process upon termination or expiration of the agreement that requires the ACO participant to furnish all data necessary to complete the annual assessment of the ACO's quality of care and addresses other relevant matters.
(b) Agreements with ACO providers/suppliers. ACOs have the option of contracting directly with its ACO providers/suppliers regarding items and services furnished to beneficiaries aligned to the ACO. For performance year 2017 and subsequent performance years, an ACO's agreement with an ACO provider/supplier regarding such items and services must satisfy the following criteria:
(1) The only parties to the agreement are the ACO and the ACO provider/supplier.
(2) The agreement must be signed by the ACO provider/supplier and by an individual who is authorized to bind the ACO.
(3) The agreement must expressly require the ACO provider/supplier to agree to participate in the Shared Savings Program and to comply with the requirements of the Shared Savings Program and all other applicable laws and regulations (including, but not limited to, those specified at § 425.208(b)).
(4) The agreement must set forth the ACO provider's/supplier's rights and obligations in, and representation by, the ACO, including without limitation, the quality reporting requirements set forth in subpart F of this part, the beneficiary notification requirements set forth at § 425.312, and how participation in the Shared Savings Program affects the ability of the ACO provider/supplier to participate in other Medicare demonstration projects or programs that involve shared savings.
(5) The agreement must describe how the opportunity to receive shared savings or other financial arrangements will encourage the ACO provider/supplier to adhere to the quality assurance and improvement program and evidence-based medicine guidelines established by the ACO.
(6) The agreement must require the ACO provider/supplier to -
(i) Update its enrollment information on a timely basis in accordance with Medicare program requirements; and
(ii) Notify the ACO of any such changes within 30 days after the change.
(7) The agreement must permit the ACO to take remedial action including the following against the ACO provider/supplier to address noncompliance with the requirements of the Shared Savings Program and other program integrity issues, including those identified by CMS:
(i) Imposition of a corrective action plan.
(ii) Denial of incentive payments.
(iii) Termination of the ACO participant agreement.
(c) Submission of agreements. The ACO must submit an executed ACO participant agreement for each ACO participant at the time of its initial application, participation agreement renewal process, and when adding to its list of ACO participants in accordance with § 425.118. The agreements may be submitted in the form and manner set forth in § 425.204(c)(6) or as otherwise specified by CMS.
[80 FR 32835, June 9, 2015]
§ 425.118 Required reporting of ACO participants and ACO providers/suppliers.
(a) List requirements.
(1) The ACO must maintain, update, and submit to CMS an accurate and complete list identifying each ACO participant (including its Medicare-enrolled TIN) and each ACO provider/supplier (including its NPI or other identifier) in accordance with this section.
(2) Before the start of an agreement period, before each performance year thereafter, and at such other times as specified by CMS, the ACO must submit to CMS an ACO participant list and an ACO provider/supplier list. The ACO may request consideration of claims billed under merged and acquired Medicare-enrolled TINs in accordance with the process set forth at § 425.204(g).
(3) The ACO must certify the submitted lists in accordance with § 425.302(a)(2).
(4) All Medicare enrolled individuals and entities that have reassigned their right to receive Medicare payment to the TIN of the ACO participant must be included on the ACO provider/supplier list and must agree to participate in the ACO and comply with the requirements of the Shared Savings Program before the ACO submits the ACO participant list and the ACO provider/supplier list.
(b) Changes to the ACO participant list —
(1) Additions.
(i) An ACO must submit to CMS a request to add an entity and its Medicare enrolled TIN to its ACO participant list. This request must be submitted at such time and in the form and manner specified by CMS.
(ii) If CMS approves the request, the entity and its Medicare enrolled TIN is added to the ACO participant list effective January 1 of the following performance year.
(iii) CMS may deny the request on the basis that the entity is not eligible to be an ACO participant or on the basis of the results of the screening performed under § 425.305(a).
(2) Deletions.
(i) An ACO must notify CMS no later than 30 days after the termination of an ACO participant agreement. Such notice must be submitted in the form and manner specified by CMS and must include the termination date of the ACO participant agreement.
(ii) The entity is deleted from the ACO participant list as of the termination date of the ACO participant agreement.
(3) Adjustments.
(i) CMS annually adjusts an ACO's assignment, historical benchmark, the quality reporting sample, and the obligation of the ACO to report on behalf of eligible professionals that bill under the TIN of an ACO participant for certain CMS quality initiatives to reflect the addition or deletion of entities from the list of ACO participants that is submitted to CMS before the start of a performance year in accordance with paragraph (a) of this section.
(ii) Absent unusual circumstances, CMS does not make adjustments during the performance year to the ACO's assignment, historical benchmark, performance year financial calculations, the quality reporting sample, or the obligation of the ACO to report on behalf of eligible professionals that bill under the TIN of an ACO participant for certain CMS quality initiatives to reflect the addition or deletion of entities from the ACO participant list that become effective during the performance year. CMS has sole discretion to determine whether unusual circumstances exist that would warrant such adjustments.
(c) Changes to the ACO provider/supplier list —
(1) Additions.
(i) An ACO must notify CMS within 30 days after an individual or entity becomes a Medicare-enrolled provider or supplier that bills for items and services it furnishes to Medicare fee-for-service beneficiaries under a billing number assigned to the TIN of an ACO participant. The notice must be submitted in the form and manner specified by CMS.
(ii) If the ACO timely submits notice to CMS, the addition of an individual or entity to the ACO provider/supplier list is effective on the date specified in the notice furnished to CMS, but no earlier than 30 days before the date of the notice. If the ACO fails to submit timely notice to CMS, the addition of an individual or entity to the ACO provider/supplier list is effective on the date of the notice.
(2) Deletions.
(i) An ACO must notify CMS no later than 30 days after an individual or entity ceases to be a Medicare-enrolled provider or supplier that bills for items and services it furnishes to Medicare fee-for-service beneficiaries under a billing number assigned to the TIN of an ACO participant. The notice must be submitted in the form and manner specified by CMS.
(ii) The deletion of an ACO provider/supplier from the ACO provider/supplier list is effective on the date the individual or entity ceased to be a Medicare-enrolled provider or supplier that bills for items and services it furnishes to Medicare fee-for-service beneficiaries under a billing number assigned to the TIN of an ACO participant.
(d) Update of Medicare enrollment information. The ACO must ensure that all changes to enrollment information for ACO participants and ACO providers/suppliers, including changes to reassignment of the right to receive Medicare payment, are reported to CMS consistent with § 424.516.
[80 FR 32836, June 9, 2015, as amended at 83 FR 68063, Dec. 31, 2018]
Subpart C - Application Procedures and Participation Agreement
§ 425.200 Participation agreement with CMS.
(a) General. In order to participate in the Shared Savings Program, an ACO must enter into a participation agreement with CMS for a period of not less than the number of years specified in this section.
(b) Agreement period.
(1) For 2012. For applications that are approved to participate in the Shared Savings Program for 2012, the start date for the participation agreement will be one of the following:
(i) April 1, 2012 (term of the participation agreement is 3 years and 9 months).
(ii) July 1, 2012 (term of the participation agreement is 3 years and 6 months).
(2) For 2013 and through 2016.
(i) The start date is January 1 of that year; and
(ii) The term of the participation agreement is 3 years unless all of the following conditions are met to extend the participation agreement by 6 months:
(A) The ACO entered an agreement period starting on January 1, 2016.
(B) The ACO elects to extend its agreement period until June 30, 2019.
(1) The ACO's election to extend its agreement period is made in the form and manner and according to the timeframe established by CMS; and
(2) An ACO executive who has the authority to legally bind the ACO must certify the election described in paragraph (b)(2)(ii)(B) of this section.
(3) For 2017 and 2018.
(i) The start date is January 1 of that year; and
(ii) The term of the participation agreement is 3 years, except as follows:
(A) For an ACO whose first agreement period in Track 1 began in 2014 or 2015, in which case the term of the ACO's initial agreement period under Track 1 (as described under § 425.604) may be extended, at the ACO's option, for an additional year for a total of 4 performance years if the conditions specified in paragraph (e) of this section are met.
(B) For an ACO whose agreement period started on January 1, 2018, the term of the participation agreement is extended by 12 months if both of the following conditions are met:
(1) The ACO elects to extend the participation agreement for a fourth performance year until December 31, 2021.
(2) The ACO's election to extend its agreement period is made in the form and manner and by a deadline established by CMS.
(4) For 2019.
(i) The start date is January 1, 2019, and the term of the participation agreement is 3 years for ACOs whose first agreement period began in 2015 and who deferred renewal of their participation agreement under paragraph (e) of this section; or
(ii) The start date is July 1, 2019, and the term of the participation agreement is 5 years and 6 months.
(5) For 2020 and subsequent years.
(i) The start date is January 1 of that year; and
(ii) The term of the participation agreement is 5 years.
(c) Performance year. The ACO's performance year under the participation agreement is the 12 month period beginning on January 1 of each year during the term of the participation agreement unless otherwise noted in its participation agreement, and except as follows:
(1) For an ACO with a start date of April 1, 2012, or July 1, 2012, the ACO's first performance year is defined as 21 months or 18 months, respectively.
(2) For an ACO that entered a first or second agreement period with a start date of January 1, 2016, and that elects to extend its agreement period by a 6-month period under paragraph (b)(2)(ii)(B) of this section, the ACO's fourth performance year is the 6-month period between January 1, 2019, and June 30, 2019.
(3) For an ACO that entered an agreement period with a start date of July 1, 2019, the ACO's first performance year of the agreement period is defined as the 6-month period between July 1, 2019, and December 31, 2019.
(d) Submission of measures. For each performance year of the agreement period, ACOs must submit measures in the form and manner required by CMS according to § 425.500(c) or § 425.510, as applicable, and as applicable according to §§ 425.608 and 425.609.
(e) Optional fourth year.
(1) To qualify for a fourth performance year as described in paragraph (b)(3)(ii) of this section, the ACO must meet all of the following conditions:
(i) The ACO's first agreement period in the Shared Savings Program under Track 1 began in 2014 or 2015.
(ii) Is currently participating in its first agreement period under Track 1.
(iii) Has requested renewal of its participation agreement in accordance with § 425.224.
(iv) Has selected a two-sided model (as described under § 425.606 or § 425.610 of this part) in its renewal request.
(v) Has requested an extension of its current agreement period and a 1-year deferral of the start of its second agreement period in a form and manner specified by CMS.
(vi) CMS approves the ACO's renewal, extension, and deferral requests.
(2) An ACO that is approved for renewal, extension, and deferral that terminates its participation agreement before the start of the first performance year of the second agreement period is—
(i) Considered to have terminated its participation agreement for the second agreement period under § 425.220; and
(ii) Not eligible to participate in the Shared Savings Program again until after the date on which the term of that second agreement period would have expired if the ACO had not terminated its participation, consistent with § 425.222.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32837, June 9, 2015; 81 FR 38013, June 10, 2016; 83 FR 60092, Nov. 23, 2018; 83 FR 68063, Dec. 31, 2018; 85 FR 27625, May 8, 2020; 85 FR 85038, Dec. 28, 2020]
§ 425.202 Application procedures.
(a) General rules.
(1) In order to obtain a determination regarding whether it meets the requirements to participate in the Shared Savings Program, a prospective ACO must submit a complete application in the form and manner required by CMS by the deadline established by CMS.
(2) An ACO executive who has the authority to legally bind the ACO must certify to the best of his or her knowledge, information, and belief that the information contained in the application is accurate, complete, and truthful.
(3) An ACO that seeks to participate in the Shared Savings Program and was newly formed after March 23, 2010, as defined in the Antitrust Policy Statement, must agree that CMS can share a copy of their application with the Antitrust Agencies.
(b) Condensed application form. For determining eligibility for agreement periods beginning before July 1, 2019:
(1) PGP demonstration sites applying to participate in the Shared Savings Program will have an opportunity to complete a condensed application form.
(2) A Pioneer ACO may use a condensed application form to apply for participation in the Shared Savings Program if it satisfies all of the following criteria:
(i) The applicant is the same legal entity as the Pioneer ACO.
(ii) The applicant's ACO participant list does not contain any ACO participant TINs that did not appear on the “Confirmed Annual TIN/NPI List” (as defined in the Pioneer ACO Model Innovation Agreement with CMS) for the applicant ACO's last full performance year in the Pioneer ACO Model.
(iii) The applicant is not applying to participate in the one-sided model.
(c) Application review. CMS reviews applications in accordance with § 425.206.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32837, June 9, 2015; 83 FR 68063, Dec. 31, 2018]
§ 425.204 Content of the application.
(a) Accountability for beneficiaries. As part of its application and participation agreement, the ACO must certify that the ACO, its ACO participants, and its ACO providers/suppliers have agreed to become accountable for the quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to the ACO.
(b) Disclosure of prior participation.
(1) The ACO must disclose to CMS whether the ACO, its ACO participants, or its ACO providers/suppliers have participated in the Medicare Shared Savings Program under the same or a different name, or is related to or has an affiliation with another Shared Savings Program ACO.
(2) The ACO must specify whether the related participation agreement is currently active or has been terminated. If it has been terminated, the ACO must specify whether the termination was voluntary or involuntary.
(3) If the ACO, ACO participant, or ACO provider/supplier was previously terminated from the Shared Savings Program, the ACO must identify the cause of termination and what safeguards are now in place to enable the ACO, ACO participant, or ACO provider/supplier to participate in the program for the full term of the participation agreement.
(c) Eligibility.
(1) As part of its application, an ACO must certify that the ACO satisfies the requirements set forth in this part. Upon request, the ACO must submit the following supporting materials to demonstrate that it satisfies the requirements set forth in this part:
(i) Documents (for example, ACO participant agreements, agreements with ACO providers/suppliers, employment contracts, and operating policies) sufficient to describe the ACO participants' and ACO providers'/suppliers' rights and obligations in and representation by the ACO, and how the opportunity to receive shared savings or other financial arrangements will encourage ACO participants and ACO providers/suppliers to adhere to the quality assurance and improvement program and evidence-based clinical guidelines.
(ii) A description, or documents sufficient to describe, how the ACO will implement the required processes and patient-centeredness criteria under § 425.112, including descriptions of the remedial processes and penalties (including the potential for expulsion) that will apply if an ACO participant or an ACO provider/supplier fails to comply with and implement these processes.
(iii) Materials documenting the ACO's organization and management structure, including an organizational chart, a list of committees (including names of committee members) and their structures, and job descriptions for senior administrative and clinical leaders specifically noted in § 425.108 and § 425.112(a)(2).
(iv) Evidence that the governing body -
(A) Is an identifiable body;
(B) Represents a mechanism for shared governance for ACO participants;
(C) Is composed of representatives of its ACO participants; and
(D) Is at least 75 percent controlled by its ACO participants.
(v) Evidence that the governing body includes a Medicare beneficiary representative(s) served by the ACO who does not have a conflict of interest with the ACO, and who has no immediate family member with conflict of interest with the ACO.
(vi) A copy of the ACO's compliance plan or documentation describing the plan that will be put in place at the time the participation agreement with CMS becomes effective.
(2) Upon request, the ACO must provide copies of all documents effectuating the ACO's formation and operation, including, without limitation the following:
(i) Charters.
(ii) By-laws.
(iii) Articles of incorporation.
(iv) Partnership agreement.
(v) Joint venture agreement.
(vi) Management or asset purchase agreements.
(vii) Financial statements and records.
(viii) Resumes and other documentation required for leaders of the ACO.
(3) If an ACO requests an exception to the governing body requirement in § 425.106(c)(2) or (c)(3), the ACO must describe -
(i) Why it seeks to differ from the requirement; and
(ii) If seeking an exception to (c)(2), how the ACO will provide meaningful representation in ACO governance by Medicare beneficiaries.
(iii) If seeking an exception to the requirement at (c)(3), why the ACO is unable to meet the requirement and how it will involve ACO participants in innovative ways in ACO governance.
(4)
(i) An ACO must certify that it is recognized as a legal entity in the State, Federal or Tribal area in which it was established and that it is authorized to conduct business in each State or Tribal area in which it operates.
(ii) An ACO formed among two or more ACO participants must provide evidence in its application that it is a legal entity separate from any of the ACO participants.
(5) The ACO must provide CMS with such information regarding its ACO participants and its ACO providers/suppliers participating in the program as is necessary to implement the program.
(i) The ACO must submit a list of all ACO participants and ACO providers/suppliers in accordance with § 425.118.
(ii) ACOs must also submit any other specific identifying information as required by CMS in the application process.
(iii) The ACO must certify the accuracy of this information.
(6) As part of the application process and upon request by CMS, the ACO must submit documents demonstrating that its ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities are required to comply with the requirements of the Shared Savings Program. The evidence to be submitted must include, without limitation, sample or form agreements and, in the case of ACO participant agreements, the first and signature page(s) of each executed ACO participant agreement. CMS may request all pages of an executed ACO participant agreement to confirm that it conforms to the sample form agreement submitted by the ACO. The ACO must certify that all of its ACO participant agreements comply with the requirements of this part.
(d) Distribution of savings. As part of its application to participate in the Shared Savings Program, an ACO must certify it has a mechanism and plan to receive and use payments for shared savings, including criteria for distributing shared savings among its ACO participants and ACO providers/suppliers.
(e) Selection of track and option for interim payment calculation.
(1) As part of its application, an ACO must specify the Track for which it is applying (as described in § 425.600).
(2)
(i) An ACO applying to participate in the program with a start date of April 1, 2012 or July 1, 2012, has the option of requesting an interim payment calculation based on the financial performance for its first 12 months of program participation and quality performance for CY 2012.
(ii) An ACO must request interim payment calculation as part of its application to participate in the Shared Savings Program.
(f) Assurance of ability to repay.
(1) An ACO must have the ability to repay all shared losses for which it may be liable under a two-sided model.
(2) An ACO that will participate in a two-sided model must establish one or more of the following repayment mechanisms in an amount and by a deadline specified by CMS in accordance with this section:
(i) An escrow account with an insured institution.
(ii) A surety bond from a company included on the U.S. Department of Treasury's List of Certified Companies.
(iii) A line of credit at an insured institution (as evidenced by a letter of credit that the Medicare program can draw upon).
(3) An ACO that will participate under a two-sided model of the Shared Savings Program must submit for CMS approval documentation that it is capable of repaying shared losses that it may incur during its agreement period, including details supporting the adequacy of the repayment mechanism.
(i) An ACO participating in Track 2 must demonstrate the adequacy of its repayment mechanism prior to any change in the terms and type of the repayment mechanism, and at such other times as requested by CMS.
(ii) An ACO entering an agreement period in Levels C, D, or E of the BASIC track or the ENHANCED track must demonstrate the adequacy of its repayment mechanism prior to the start of its agreement period, prior to any change in the terms and type of the repayment mechanism, and at such other times as requested by CMS.
(iii) An ACO entering an agreement period in Level A or Level B of the BASIC track must demonstrate the adequacy of its repayment mechanism prior to the start of any performance year in which it either elects to participate in, or is automatically transitioned to, a two-sided model, Level C, Level D, or Level E of the BASIC track, prior to any change in the terms and type of the repayment mechanism, and at such other times as requested by CMS.
(iv) An ACO that has submitted a request to renew its participation agreement must submit as part of the renewal request documentation demonstrating the adequacy of the repayment mechanism that could be used to repay any shared losses incurred for performance years in the next agreement period. The repayment mechanism applicable to the new agreement period may be the same repayment mechanism currently used by the ACO, provided that the ACO submits documentation establishing that the duration of the existing repayment mechanism has been revised to comply with paragraph (f)(6)(ii) of this section, and the amount of the repayment mechanism complies with paragraph (f)(4) of this section.
(v) As part of its application, a re-entering ACO must submit documentation demonstrating the adequacy of the repayment mechanism that could be used to repay any shared losses incurred for performance years in the next agreement period. The repayment mechanism applicable to the new agreement period may be the same repayment mechanism currently used by the re-entering ACO, provided that the ACO is the same legal entity as an ACO that previously participated in the program, and the ACO submits documentation establishing that the duration of the existing repayment mechanism has been revised to comply with paragraph (f)(6)(ii) of this section and the amount of the repayment mechanism complies with paragraph (f)(4) of this section.
(4) CMS calculates the amount of the repayment mechanism as follows:
(i) For a Track 2 ACO, the repayment mechanism amount must be equal to at least 1 percent of the total per capita Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries, based on expenditures used to calculate the benchmark for the applicable agreement period, as estimated by CMS at the time of application.
(ii) For a BASIC track or ENHANCED track ACO, the repayment mechanism amount must be equal to the lesser of the following:
(A) One percent of the total per capita Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries, based on expenditures for the most recent calendar year for which 12 months of data are available.
(B) Two percent of the total Medicare Parts A and B fee-for-service revenue of its ACO participants, based on revenue for the most recent calendar year for which 12 months of data are available.
(iii) For agreement periods beginning on or after July 1, 2019, CMS recalculates the ACO's repayment mechanism amount before the second and each subsequent performance year in the agreement period in accordance with this section based on the certified ACO participant list for the relevant performance year.
(A) If the recalculated repayment mechanism amount exceeds the existing repayment mechanism amount by at least 50 percent or $1,000,000, whichever is the lesser value, CMS notifies the ACO in writing that the amount of its repayment mechanism must be increased to the recalculated repayment mechanism amount.
(B) Within 90 days after receipt of such written notice from CMS, the ACO must submit for CMS approval documentation that the amount of its repayment mechanism has been increased to the amount specified by CMS.
(iv)
(A) In the case of an ACO that has submitted a request to enter a new participation agreement for an agreement period starting on or after January 1, 2022 and is a renewing ACO or a re-entering ACO that is the same legal entity as an ACO that previously participated in the program: If the ACO wishes to use its existing repayment mechanism to establish its ability to repay any shared losses incurred for performance years in the new agreement period, the amount of the repayment mechanism must be equal to at least the amount calculated by CMS in accordance with paragraph (f)(4)(ii) of this section.
(B) Under the following circumstances, an ACO that renewed its participation agreement for an agreement period beginning on July 1, 2019, or January 1, 2020, may elect to decrease the amount of its repayment mechanism.
(1) The ACO elected to continue to use its existing repayment mechanism for the agreement period beginning on July 1, 2019, or January 1, 2020, and the amount of that repayment mechanism was greater than the repayment mechanism amount estimated at the time of renewal application according to paragraph (f)(4)(ii) of this section.
(2) The repayment mechanism amount for performance year 2021, as recalculated pursuant to paragraph (f)(4)(iii) of this section, is less than the existing repayment mechanism amount.
(3) CMS will notify the ACO in writing if the ACO may elect to decrease the amount of its repayment mechanism pursuant to this paragraph (f)(4)(iv)(B). The ACO must submit such election, together with revised repayment mechanism documentation, in a form and manner and by a deadline specified by CMS. CMS will review the revised repayment mechanism documentation and may reject the election if the repayment mechanism documentation does not comply with the requirements of this paragraph (f).
(5) After the repayment mechanism has been used to repay any portion of shared losses owed to CMS, the ACO must replenish the amount of funds available through the repayment mechanism within 90 days. The resulting amount available through the repayment mechanism must be at least the amount specified by CMS in accordance with paragraph (f)(4) of this section.
(6) The repayment mechanism must be in effect for the duration of the ACO's participation under a two-sided model plus 12 months following the conclusion of the agreement period, except as otherwise specified in this section.
(i) For an ACO that is establishing a new repayment mechanism to meet this requirement, the repayment mechanism must satisfy one of the following criteria:
(A) The repayment mechanism covers the entire duration of the ACO's participation under a two-sided risk model plus 12 months following the conclusion of the agreement period.
(B) The repayment mechanism covers a term of at least the first two performance years in which the ACO is participating under a two-sided model and provides for automatic, annual 12-month extensions of the repayment mechanism such that the repayment mechanism will eventually remain in effect for the duration of the agreement period plus 12 months following the conclusion of the agreement period.
(ii) For a renewing ACO, or a re-entering ACO that is the same legal entity as an ACO that previously participated in the program, that wishes to use its existing repayment mechanism to establish its ability to repay any shared losses incurred for performance years in the new agreement period, the existing repayment mechanism must be amended to meet one of the following criteria.
(A) The duration of the existing repayment mechanism is extended by an amount of time that covers the duration of the new agreement period plus 12 months following the conclusion of the new agreement period.
(B) The duration of the existing repayment mechanism is extended, if necessary, to cover a term of at least the first two performance years of the new agreement period and provides for automatic, annual 12-month extensions of the repayment mechanism such that the repayment mechanism will eventually remain in effect for the duration of the new agreement period plus 12 months following the conclusion of the new agreement period.
(iii) CMS may require the ACO to extend the duration of the repayment mechanism if necessary to ensure that the ACO fully repays CMS any shared losses for each of the performance years of the agreement period.
(iv) The repayment mechanism may be terminated at the earliest of the following conditions:
(A) The ACO has fully repaid CMS any shared losses owed for each of the performance years of the agreement period under a two-sided model.
(B) CMS has exhausted the amount reserved by the ACO's repayment mechanism and the arrangement does not need to be maintained to support the ACO's participation under the Shared Savings Program.
(C) CMS determines that the ACO does not owe any shared losses under the Shared Savings Program for any of the performance years of the agreement period.
(g) Consideration of claims billed under merged and acquired entities' TINs. An ACO may request that CMS consider, for purposes of beneficiary assignment and establishing the ACO's benchmark under § 425.601, § 425.602, or § 425.603, claims billed under the TINs of entities that have been acquired through sale or merger by an ACO participant.
(1) The ACO may include an acquired entity's TIN on its ACO participant list under the following circumstances:
(i) The ACO participant has subsumed the acquired entity's TIN in its entirety, including all of the providers and suppliers that reassigned their right to receive Medicare payment to the acquired entity's TIN.
(ii) Each provider or supplier that previously reassigned his or her right to receive Medicare payment to the acquired entity's TIN has reassigned his or her right to receive Medicare payment to the TIN of the acquiring ACO participant and has been added to the ACO provider/supplier list under paragraph (c)(5) of the section.
(iii) The acquired entity's TIN is no longer used to bill Medicare.
(2) The ACO must submit the following supporting documentation in the form and manner specified by CMS.
(i) An attestation that -
(A) Identifies by TIN both the acquired entity and the ACO participant that acquired it;
(B) Specifies that all the providers and suppliers that previously reassigned their right to receive Medicare payment to the acquired entity's TIN have reassigned such right to the TIN of the identified ACO participant and have been added to the ACO provider/supplier list under paragraph (c)(5) of this section; and
(C) Specifies that the acquired entity's TIN is no longer used to bill Medicare.
(ii) Documentation sufficient to demonstrate that the acquired entity's TIN was merged with or purchased by the ACO participant.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32837, June 9, 2015; 81 FR 80559, Nov. 15, 2016; 82 FR 53369, Nov. 15, 2017; 83 FR 68063, Dec. 31, 2018; 85 FR 85038, Dec. 28, 2020]
§ 425.206 Evaluation procedures for applications.
(a) Basis for evaluation and determination.
(1) CMS evaluates an ACO's application to determine whether an applicant satisfies the requirements of this part and is qualified to participate in the Shared Savings Program, and approves or denies applications accordingly. Applications are approved or denied on the basis of the following:
(i) Information contained in and submitted with the application by an application deadline specified by CMS.
(ii) Supplemental information that was submitted in response to a CMS request and by a deadline specified by CMS.
(iii) Other information available to CMS.
(2) CMS notifies an ACO applicant when supplemental information is required for CMS to make a determination on the ACO's application and provides an opportunity for the ACO to submit the information.
(3) CMS may deny an application if an ACO applicant fails to submit requested information by the deadlines established by CMS.
(b) Notice of determination.
(1) CMS notifies in writing each applicant ACO of its determination to approve or deny the ACO's application to participate in the Shared Savings Program.
(2) If CMS denies the application, the notice will indicate that the ACO is not qualified to participate in the Shared Savings Program, specify the reasons why the ACO is not so qualified, and inform the ACO of its right to request reconsideration review in accordance with the procedures specified in subpart I of this part.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32838, June 9, 2015]
§ 425.208 Provisions of participation agreement.
(a) General rules.
(1) Upon being notified by CMS of its approval to participate in the Shared Savings Program, an executive of that ACO who has the ability to legally bind the ACO must sign and submit to CMS a participation agreement.
(2) Under the participation agreement the ACO must agree to comply with the provisions of this part in order to participate in the Shared Savings Program.
(b) Compliance with laws. The ACO must agree, and must require its ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to the ACO's activities to agree, or to comply with all applicable laws including, but not limited to, the following:
(1) Federal criminal law.
(2) The False Claims Act (31 U.S.C. 3729 et seq.).
(3) The anti-kickback statute (42 U.S.C. 1320a-7b(b)).
(4) The civil monetary penalties law (42 U.S.C. 1320a-7a).
(5) The physician self-referral law (42 U.S.C. 1395nn).
(c) Certifications.
(1) The ACO must agree, as a condition of participating in the program and receiving any shared savings payment, that an individual with the authority to legally bind the ACO will certify the accuracy, completeness, and truthfulness of any data or information requested by or submitted to CMS, including, but not limited to, the application form, participation agreement, and any quality data or other information on which CMS bases its calculation of shared savings payments and shared losses.
(2) Certifications must meet the requirements at § 425.302.
§ 425.210 Application of agreement to ACO participants, ACO providers/suppliers, and others.
(a) The ACO must provide a copy of its participation agreement with CMS to all ACO participants, ACO providers/suppliers, and other individuals and entities involved in ACO governance.
(b) All contracts or arrangements between or among the ACO, ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities must require compliance with the requirements and conditions of this part, including, but not limited to, those specified in the participation agreement with CMS.
§ 425.212 Changes to program requirements during the agreement period.
(a) An ACO is subject to all regulatory changes that become effective during the agreement period, with the exception of the following program areas, unless otherwise required by statute:
(1) Eligibility requirements concerning the structure and governance of ACOs.
(2) Calculation of sharing rate.
(b) In those instances where there are changes in law or regulations, the ACO will be required to submit to CMS for review and approval, as a supplement to its original application, an explanation detailing how it will modify its processes to address these changes in law or regulations.
(c) If an ACO does not modify its processes to address a change in law or regulations, it will be placed on a CAP. If the ACO fails to effectuate the necessary modifications while under the CAP, the ACO will be terminated from the Shared Savings Program using the procedures in § 425.218.
(d) An ACO will be permitted to terminate its agreement, in those instances where Shared Savings Program statutory and regulatory standards are established during the agreement period which the ACO believes will impact its ability to continue to participate in the Shared Savings Program.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32838, June 9, 2015]
§ 425.214 Managing changes to the ACO during the agreement period.
(a)
(1) An ACO must notify CMS within 30 days of any significant change.
(2) An ACO's failure to notify CMS of a significant change does not preclude CMS from determining that the ACO has experienced a significant change.
(3) A “significant change” occurs when an ACO is no longer able to meet the eligibility or program requirements of this part.
(b) Upon becoming aware of a significant change or receiving an ACO's notice of a significant change described in paragraph (b) of this section, CMS reevaluates the ACO's eligibility to continue to participate in the Shared Savings Program and may request additional documentation. CMS may make a determination that includes one of the following:
(1) The ACO may continue to operate under the new structure.
(2) The ACO structure is so different from the initially approved ACO that it must terminate its participation agreement and submit a new application for participation.
(3) The ACO no longer meets the eligibility criteria for the program and its participation agreement must be terminated.
(4) CMS and the ACO may mutually decide to terminate the participation agreement.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32838, June 9, 2015]
§ 425.216 Actions prior to termination.
(a) Pre-termination actions.
(1) If CMS concludes that termination of an ACO from the Shared Savings Program is warranted, CMS may take one or more of the following actions prior to termination of the ACO from the Shared Savings Program.
(i) Provide a warning notice to the ACO regarding noncompliance with one or more program requirements.
(ii) Request a CAP from the ACO.
(iii) Place the ACO on a special monitoring plan.
(2) Nothing in this part, including the actions set forth in paragraph (a)(1) of this section, negates, diminishes, or otherwise alters the applicability of other laws, rules, or regulations, including, but not limited to, the Sherman Act (15 U.S.C. 1 et seq.), the Clayton Act (15 U.S.C. 12), and the Federal Trade Commission Act (15 U.S.C. 45 et seq.).
(b) Corrective action plans.
(1) The ACO must submit a CAP for CMS approval by the deadline indicated on the notice of violation.
(i) The CAP must address what actions the ACO will take to ensure that the ACO, ACO participants, ACO providers/suppliers or other individuals or entities performing functions or services related to the ACO's activities or both correct any deficiencies and comply with all applicable Shared Savings Program requirements.
(ii) The ACO's performance will be monitored and evaluated during and after the CAP process.
(2) CMS may terminate the participation agreement if the ACO fails to submit, obtain approval for, or implement a CAP, or fails to demonstrate improved performance upon completion of the CAP.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32839, June 9, 2015]
§ 425.218 Termination of the participation agreement by CMS.
(a) General. CMS may terminate the participation agreement with an ACO when an ACO, the ACO participants, ACO providers/suppliers or other individuals or entities performing functions or services related to ACO activities fail to comply with any of the requirements of the Shared Savings Program under this part.
(b) Grounds for termination by CMS. CMS may terminate the participation agreement for reasons including, but not limited to the following:
(1) Non-compliance with eligibility and other requirements described in this part.
(2) The imposition of sanctions or other actions taken against the ACO by an accrediting organization, State, Federal or local government agency leading to inability of the ACO to comply with the requirements under this part.
(3) Violations of the physician self-referral prohibition, civil monetary penalties (CMP) law, Federal anti-kickback statute, antitrust laws, or any other applicable Medicare laws, rules, or regulations that are relevant to ACO operations.
(4) Failure to comply with CMS requests for documentation or other information by the deadline specified by CMS.
(5) Submitting false or fraudulent data or information.
(c) CMS may immediately terminate a participation agreement without taking any of the pre-termination actions set forth in § 425.216.
(d) Notice of termination by CMS. CMS notifies an ACO in writing of its decision to terminate the participation agreement.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32839, June 9, 2015]
§ 425.220 Termination of the participation agreement by the ACO.
(a) Notice of termination. An ACO must provide at least 30 days advance written notice to CMS and its ACO participants of its decision to terminate the participation agreement and the effective date of its termination.
(b) [Reserved]
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32839, June 9, 2015; 83 FR 68064, Dec. 31, 2018]
§ 425.221 Close-out procedures and payment consequences of early termination.
(a) Close-out procedures.
(1) An ACO whose participation agreement has expired or is terminated by CMS under § 425.218 or by the ACO under § 425.220 must implement close-out procedures including but not limited to the following issues in a form and manner and by a deadline specified by CMS:
(i) Notice to ACO participants of termination.
(ii) Record retention.
(iii) Data sharing.
(iv) Quality reporting.
(v) Beneficiary continuity of care.
(2) ACOs that fail to complete close-out procedures in the form and manner and by the deadline specified by CMS will not be eligible to share in savings.
(b) Payment consequences of early termination.
(1) Receipt of shared savings.
(i) Except as set forth in paragraph (b)(3)(i) of this section, an ACO that terminates its participation agreement under § 425.220 is eligible to receive shared savings for the performance year during which the termination becomes effective only if all of the following conditions are met:
(A) CMS designates or approves an effective date of termination of the last calendar day of the performance year.
(B) The ACO has completed all close-out procedures by the deadline specified by CMS.
(C) The ACO has satisfied the criteria for sharing in savings for the performance year.
(ii) If the participation agreement is terminated at any time by CMS under § 425.218, the ACO is not eligible to receive shared savings for the performance year during which the termination becomes effective.
(2) Payment of shared losses.
(i) Except as set forth in paragraph (b)(3)(i) of this section, for performance years beginning before July 1, 2019, an ACO under a two-sided model is not liable for any shared losses if its participation agreement is terminated effective before the last calendar day of a performance year.
(ii) Except as set forth in paragraph (b)(3)(ii) of this section, for performance years beginning on July 1, 2019 and subsequent performance years, an ACO under a two-sided model is liable for a pro-rated share of any shared losses, as calculated in paragraph (b)(2)(iii) of this section, if its participation agreement is terminated effective before the last calendar day of a performance year.
(A) An ACO under a two-sided model that terminates its participation agreement under § 425.220 with an effective date of termination after June 30th of a 12-month performance year is liable for a pro-rated share of any shared losses determined for the performance year during which the termination becomes effective.
(B) An ACO under a two-sided model whose participation agreement is terminated by CMS under § 425.218 is liable for a pro-rated share of any shared losses determined for the performance year during which the termination becomes effective.
(iii) The pro-rated share of losses described in paragraph (b)(2)(ii) of this section is calculated as follows:
(A) In the case of a 12-month performance year, the shared losses incurred during the 12 months of the performance year are multiplied by the quotient equal to the number of months of participation in the program during the performance year, including the month in which the termination was effective, divided by 12.
(B) In the case of a 6-month performance year beginning July 1, 2019, the shared losses incurred during CY 2019 are multiplied by the quotient equal to the number of months of participation in the program during the performance year, including the month in which the termination was effective, divided by 12.
(3) Exceptions.
(i) An ACO starting a 12-month performance year on January 1, 2019, that terminates its participation agreement with an effective date of termination of June 30, 2019, and that enters a new agreement period beginning on July 1, 2019, is eligible for pro-rated shared savings or liable for pro-rated shared losses for the 6-month period from January 1, 2019, through June 30, 2019, as determined in accordance with § 425.609.
(ii) An ACO under a two-sided model that terminates its participation agreement under § 425.220 during the 6-month performance year beginning July 1, 2019, with an effective date of termination prior to the last calendar day of the performance year is not liable for shared losses incurred during the performance year.
[80 FR 32839, June 9, 2015, as amended at 83 FR 60092, Nov. 23, 2018; 83 FR 68064, Dec. 31, 2018]
§ 425.222 Eligibility to re-enter the program for agreement periods beginning before July 1, 2019.
(a) For purposes of determining the eligibility of a re-entering ACO to enter an agreement period beginning before July 1, 2019, the ACO may participate in the Shared Savings Program again only after the date on which the term of its original participation agreement would have expired if the ACO had not been terminated.
(b) For purposes of determining the eligibility of a re-entering ACO to enter an agreement period beginning before July 1, 2019, an ACO whose participation agreement was previously terminated must demonstrate in its application that it has corrected the deficiencies that caused it to be terminated from the Shared Savings Program and has processes in place to ensure that it remains in compliance with the terms of the new participation agreement.
(c) For purposes of determining the eligibility of a re-entering ACO to enter an agreement period beginning before July 1, 2019, an ACO whose participation agreement was previously terminated or expired without having been renewed may re-enter the program for a subsequent agreement period.
(1) If the termination occurred less than half way through the agreement period, an ACO that was previously under a one-sided model may reenter the program under the one-sided model or a two-sided model. If the ACO reenters the program under the one-sided model, the ACO will be considered to be in the same agreement period under the one-sided model as it was at the time of termination.
(2) If the termination occurred more than half way through the agreement period, an ACO that was previously in its first agreement period under the one-sided model may reenter the program under the one-sided model or a two-sided model. If the ACO reenters the program under the one-sided model, the ACO will be considered to be in its second agreement period under the one-sided model. An ACO that was previously in its second agreement period under the one-sided model must reenter the program under a two-sided model.
(3) Regardless of the date of termination, an ACO that was previously under a two-sided model may only reapply for participation in a two-sided model.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32839, June 9, 2015; 83 FR 68065, Dec. 31, 2018]
§ 425.224 Application procedures for renewing ACOs and re-entering ACOs.
(a) General rules. A renewing ACO or a re-entering ACO may apply to enter a new participation agreement with CMS for participation in the Shared Savings Program.
(1) In order to obtain a determination regarding whether it meets the requirements to participate in the Shared Savings Program, the ACO must submit a complete application in the form and manner and by the deadline specified by CMS.
(2) An ACO executive who has the authority to legally bind the ACO must certify to the best of his or her knowledge, information, and belief that the information contained in the application is accurate, complete, and truthful.
(3) An ACO that seeks to enter a new participation agreement under the Shared Savings Program and was newly formed after March 23, 2010, as defined in the Antitrust Policy Statement, must agree that CMS can share a copy of its application with the Antitrust Agencies.
(4) The ACO must select a participation option in accordance with the requirements specified in § 425.600. Regardless of the date of termination or expiration of the participation agreement, a renewing ACO or re-entering ACO that was previously under a two-sided model, or a one-sided model of the BASIC track's glide path (Level A or Level B), may only reapply for participation in a two-sided model.
(b) Review of application.
(1) CMS determines whether to approve a renewing ACO's or re-entering ACO's application based on an evaluation of all of the following factors:
(i) Whether the ACO satisfies the criteria for operating under the selected risk track.
(ii) The ACO's history of noncompliance with the requirements of the Shared Savings Program, including, but not limited to, the following factors:
(A) Whether the ACO demonstrated a pattern of failure to meet the quality performance standards or met any of the criteria for termination under § 425.316(c)(1)(ii) or (c)(2)(ii).
(B) For 2 performance years of the ACO's previous agreement period, regardless of whether the years are in consecutive order, whether the average per capita Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiary population exceeded its updated benchmark by an amount equal to or exceeding either of the following:
(1) The ACO's negative MSR, under a one-sided model.
(2) The ACO's MLR, under a two-sided model.
(C) Whether the ACO failed to repay shared losses in full within 90 days as required under subpart G of this part for any performance year of the ACO's previous agreement period in a two-sided model.
(D) For an ACO that has participated in a two-sided model authorized under section 1115A of the Act, whether the ACO failed to repay shared losses for any performance year as required under the terms of the ACO's participation agreement for such model.
(iii) Whether the ACO has demonstrated in its application that it has corrected the deficiencies that caused any noncompliance identified in paragraph (b)(1)(ii) of this section to occur, and any other factors that may have caused the ACO to be terminated from the Shared Savings Program, and has processes in place to ensure that it remains in compliance with the terms of the new participation agreement.
(iv) Whether the ACO has established that it is in compliance with the eligibility and other requirements of the Shared Savings Program to enter a new participation agreement, including the ability to repay losses by establishing an adequate repayment mechanism under § 425.204(f), if applicable.
(v) The results of a program integrity screening of the ACO, its ACO participants, and its ACO providers/suppliers (conducted in accordance with § 425.305(a)).
(2) Applications are approved or denied on the basis of the following information:
(i) Information contained in and submitted with the application by a deadline specified by CMS.
(ii) Supplemental information that was submitted by a deadline specified by CMS in response to a CMS request for information.
(iii) Other information available to CMS.
(3) CMS notifies the ACO when supplemental information is required for CMS to make such a determination and provides an opportunity for the ACO to submit the information.
(c) Notice of determination.
(1) CMS notifies the ACO in writing of its determination to approve or deny the ACO's application.
(2) If CMS denies the application, the notice of determination -
(i) Specifies the reasons for the denial; and
(ii) Informs the ACO of its right to request reconsideration review in accordance with the procedures specified in subpart I of this part.
[80 FR 32839, June 9, 2015, as amended at 83 FR 68065, Dec. 31, 2018; 85 FR 85039, Dec. 28, 2020]
§ 425.226 Annual participation elections.
(a) General. This section applies to ACOs in agreement periods beginning on July 1, 2019, and in subsequent years. Before the start of a performance year, an ACO may make elections related to its participation in the Shared Savings Program, as specified in this section, effective at the start of the applicable performance year and for the remaining years of the agreement period, unless superseded by a later election in accordance with this section.
(1) Selection of beneficiary assignment methodology. An ACO may select the assignment methodology that CMS employs for assignment of beneficiaries under subpart E of this part. An ACO may select either of the following:
(i) Preliminary prospective assignment with retrospective reconciliation, as described in § 425.400(a)(2).
(ii) Prospective assignment, as described in § 425.400(a)(3).
(2) Selection of BASIC track level. An ACO participating under the BASIC track in the glide path may select a higher level of risk and potential reward, as provided in this section.
(i) An ACO participating under the BASIC track's glide path may elect to transition to a higher level of risk and potential reward within the glide path than the level of risk and potential reward that the ACO would be automatically transitioned to in the applicable year as specified in § 425.605(d)(1). The automatic transition to higher levels of risk and potential reward within the BASIC track's glide path continues to apply to all subsequent years of the agreement period in the BASIC track.
(ii) An ACO transitioning to a higher level of risk and potential reward under paragraph (a)(2)(i) of this section must meet all requirements to participate under the selected level of performance-based risk, including both of the following:
(A) Establishing an adequate repayment mechanism as specified under § 425.204(f).
(B) Selecting a MSR/MLR from the options specified under § 425.605(b).
(b) Election procedures.
(1) All annual elections must be made in a form and manner and according to the timeframe established by CMS.
(2) ACO executive who has the authority to legally bind the ACO must certify the elections described in this section.
[83 FR 68066, Dec. 31, 2018]
Subpart D - Program Requirements and Beneficiary Protections
§ 425.300 Compliance plan.
(a) The ACO must have a compliance plan that includes at least the following elements:
(1) A designated compliance official or individual who is not legal counsel to the ACO and reports directly to the ACO's governing body.
(2) Mechanisms for identifying and addressing compliance problems related to the ACO's operations and performance.
(3) A method for employees or contractors of the ACO, ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities to anonymously report suspected problems related to the ACO to the compliance officer.
(4) Compliance training for the ACO, the ACO participants, and the ACO providers/suppliers.
(5) A requirement for the ACO to report probable violations of law to an appropriate law enforcement agency.
(b)
(1) ACOs that are existing entities may use the current compliance officer if the compliance officer meets the requirements set forth in paragraph (a)(1) of this section.
(2) An ACO's compliance plan must be in compliance with and be updated periodically to reflect changes in law and regulations.
§ 425.302 Program requirements for data submission and certifications.
(a) Requirements for data submission and certification.
(1) The ACO, its ACO participants, its ACO providers/suppliers or individuals or other entities performing functions or services related to ACO activities must submit all data and information, including data on measures designated by CMS under § 425.500 or § 425.510, as applicable, in a form and manner specified by CMS.
(2) Certification of data upon submission. With respect to data and information that are generated or submitted by the ACO, ACO participants, ACO providers/suppliers, or other individuals or entities performing functions or services related to ACO activities, an individual with the authority to legally bind the individual or entity submitting such data or information must certify the accuracy, completeness, and truthfulness of the data and information to the best of his or her knowledge information and belief.
(3) Annual certification. At the end of each performance year, an individual with the legal authority to bind the ACO must certify to the best of his or her knowledge, information, and belief -
(i) That the ACO, its ACO participants, its ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities are in compliance with program requirements;
(ii) The accuracy, completeness, and truthfulness of all data and information that are generated or submitted by the ACO, ACO participants, ACO providers/suppliers, or other individuals or entities performing functions or services related to ACO activities, including any quality data or other information or data relied upon by CMS in determining the ACO's eligibility for, and the amount of a shared savings payment or the amount of shared losses or other monies owed to CMS; and
(iii) That the percentage of eligible clinicians participating in the ACO that use CEHRT to document and communicate clinical care to their patients or other health care providers meets or exceeds the applicable percentage specified by CMS at § 425.506(f).
(b) [Reserved]
[76 FR 67973, Nov. 2, 2011, as amended at 83 FR 60092, Nov. 23, 2018; 85 FR 85039, Dec. 28, 2020]
§ 425.304 Beneficiary incentives.
(a) General.
(1) Except as set forth in this section, or as otherwise permitted by law, ACOs, ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities are prohibited from providing gifts or other remuneration to beneficiaries as inducements for receiving items or services from or remaining in, an ACO or with ACO providers/suppliers in a particular ACO or receiving items or services from ACO participants or ACO providers/suppliers.
(2) Nothing in this section shall be construed as prohibiting an ACO from using shared savings received under this part to cover the cost of an in-kind item or service or incentive payment provided to a beneficiary under paragraph (b) or (c) of this section.
(b) In-kind incentives. ACOs, ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities may provide in-kind items or services to Medicare fee-for-service beneficiaries if all of the following conditions are satisfied:
(1) There is a reasonable connection between the items and services and the medical care of the beneficiary.
(2) The items or services are preventive care items or services or advance a clinical goal for the beneficiary, including adherence to a treatment regime, adherence to a drug regime, adherence to a follow-up care plan, or management of a chronic disease or condition.
(3) The in-kind item or service is not a Medicare-covered item or service for the beneficiary on the date the in-kind item or service is furnished to the beneficiary.
(c) Monetary incentives —
(1) General. For performance years beginning on July 1, 2019 and for subsequent performance years, an ACO that is participating under Track 2, Levels C, D, or E of the BASIC track, or the ENHANCED track may, in accordance with this section, establish a beneficiary incentive program to provide monetary incentive payments to Medicare fee-for-service beneficiaries who receive a qualifying service.
(2) Application procedures.
(i) To establish or reestablish a beneficiary incentive program, an ACO must submit a complete application in the form and manner and by a deadline specified by CMS.
(ii) CMS evaluates an ACO's application to determine whether the ACO satisfies the requirements of this section, and approves or denies the application.
(iii) If an ACO wishes to make a material change to its CMS-approved beneficiary incentive program, the ACO must submit a description of the material change to CMS in a form and manner and by a deadline specified by CMS. CMS will promptly evaluate the proposed material change and approve or reject it.
(3) Beneficiary incentive program requirements. An ACO must begin to operate its approved beneficiary incentive program beginning on July 1, 2019 or January 1 of the relevant performance year.
(i) Duration.
(A) Subject to the termination provision at paragraph (c)(7) of this section, an ACO must operate its approved beneficiary incentive program for an initial period of 18 months in the case of an ACO approved to operate a beneficiary incentive program beginning on July 1, 2019, or 12 months in the case of an ACO approved to operate a beneficiary incentive program beginning on January 1 of a performance year.
(B) For each consecutive year that an ACO wishes to operate its beneficiary incentive program after the CMS-approved initial period, it must certify all of the following by a deadline specified by CMS:
(1) Its intent to continue to operate the beneficiary incentive program for the entirety of the relevant performance year.
(2) That the beneficiary incentive program meets all applicable requirements.
(ii) Beneficiary eligibility. A fee-for-service beneficiary is eligible to receive an incentive payment under a beneficiary incentive program if the beneficiary is assigned to the ACO through either of the following:
(A) Preliminary prospective assignment, as described in § 425.400(a)(2).
(B) Prospective assignment, as described in § 425.400(a)(3).
(iii) Qualifying service. For purposes of this section, a qualifying service is a primary care service (as defined in § 425.20) with respect to which coinsurance applies under Part B, if the service is furnished through an ACO by one of the following:
(A) An ACO professional who has a primary care specialty designation included in the definition of primary care physician under § 425.20.
(B) An ACO professional who is a physician assistant, nurse practitioner, or certified nurse specialist.
(C) A FQHC or RHC.
(iv) Incentive payments.
(A) An ACO that establishes a beneficiary incentive program must furnish an incentive payment for each qualifying service furnished to a beneficiary described in paragraph (c)(3)(ii) of this section in accordance with this section.
(B) Each incentive payment made by an ACO under a beneficiary incentive program must satisfy all of the following conditions:
(1) The incentive payment is in the form of a check, debit card, or a traceable cash equivalent.
(2) The value of the incentive payment does not exceed $20, as adjusted annually by the percentage increase in the consumer price index for all urban consumers (United States city average) for the 12-month period ending with June of the previous year, rounded to the nearest whole dollar amount.
(3) The incentive payment is provided by the ACO to the beneficiary no later than 30 days after a qualifying service is furnished.
(C) An ACO must furnish incentive payments in the same amount to each eligible Medicare fee-for-service beneficiary without regard to enrollment of such beneficiary in a Medicare supplemental policy (described in section 1882(g)(1) of the Act), in a State Medicaid plan under title XIX or a waiver of such a plan, or in any other health insurance policy or health benefit plan.
(4) Program integrity requirements —
(i) Record retention. An ACO that establishes a beneficiary incentive program must maintain records related to the beneficiary incentive program that include the following:
(A) Identification of each beneficiary that received an incentive payment, including beneficiary name and HICN or Medicare beneficiary identifier.
(B) The type and amount of each incentive payment made to each beneficiary.
(C) The date each beneficiary received a qualifying service, the corresponding HCPCS code for the qualifying service, and identification of the ACO provider/supplier that furnished the qualifying service.
(D) The date the ACO provided each incentive payment to each beneficiary.
(ii) Source of funding.
(A) An ACO must not use funds from any entity or organization outside of the ACO to establish or operate a beneficiary incentive program.
(B) An ACO must not directly, through insurance, or otherwise, bill or otherwise shift the cost of establishing or operating a beneficiary incentive program to a Federal health care program.
(iii) Beneficiary notifications. An ACO or its ACO participants shall notify assigned beneficiaries of the availability of the beneficiary incentive program in accordance with § 425.312(b).
(iv) Marketing prohibition. Except for the beneficiary notifications required under this section, the beneficiary incentive program is not the subject of marketing materials and activities, including but not limited to, an advertisement or solicitation to a beneficiary or any potential patient whose care is paid for in whole or in part by a Federal health care program (as defined at 42 U.S.C. 1320a-7b(f)).
(5) Effect on program calculations. CMS disregards incentive payments made by an ACO under paragraph (c) of this section in calculating an ACO's benchmarks, estimated average per capita Medicare expenditures, and shared savings and losses.
(6) Income exemptions. Incentive payments made under a beneficiary incentive program are not considered income or resources or otherwise taken into account for purposes of either of the following:
(i) Determining eligibility for benefits or assistance (or the amount or extent of benefits or assistance) under any Federal program or under any State or local program financed in whole or in part with Federal funds.
(ii) Any Federal or State laws relating to taxation.
(7) Termination. CMS may require an ACO to terminate its beneficiary incentive program at any time for either of the following:
(i) Failure to comply with the requirements of this section.
(ii) Any of the grounds for ACO termination set forth in § 425.218(b).
[83 FR 68066, Dec. 31, 2018]
§ 425.305 Other program safeguards.
(a) Screening of ACO applicants.
(1) ACOs, ACO participants, and ACO providers/suppliers are reviewed during the Shared Savings Program application process and periodically thereafter with regard to their program integrity history, including any history of Medicare program exclusions or other sanctions and affiliations with individuals or entities that have a history of program integrity issues.
(2) ACOs, ACO participants, or ACO providers/suppliers whose screening reveals a history of program integrity issues or affiliations with individuals or entities that have a history of program integrity issues may be subject to denial of their Shared Savings Program applications or the imposition of additional safeguards or assurances against program integrity risks.
(b) Prohibition on certain required referrals and cost shifting. ACOs, ACO participants, and ACO providers/suppliers are prohibited from doing the following:
(1) Conditioning the participation of ACO participants, ACO providers/suppliers, other individuals or entities performing functions or services related to ACO activities in the ACO on referrals of Federal health care program business that the ACO, its ACO participants, or ACO providers/suppliers or other individuals or entities performing functions or services related to ACO activities know or should know is being (or would be) provided to beneficiaries who are not assigned to the ACO.
(2) Requiring that beneficiaries be referred only to ACO participants or ACO providers/suppliers within the ACO or to any other provider or supplier, except that the prohibition does not apply to referrals made by employees or contractors who are operating within the scope of their employment or contractual arrangement to the employer or contracting entity, provided that the employees and contractors remain free to make referrals without restriction or limitation if the beneficiary expresses a preference for a different provider, practitioner, or supplier; the beneficiary's insurer determines the provider, practitioner, or supplier; or the referral is not in the beneficiary's best medical interests in the judgment of the referring party.
[83 FR 68067, Dec. 31, 2018]
§ 425.306 Participant agreement and exclusivity of ACO participants.
(a) Each ACO participant must commit to the term of the participation agreement and sign an ACO participant agreement that complies with the requirements of this part.
(b)
(1) Except as specified in paragraph (b)(2) of this section, ACO participants are not required to be exclusive to one Shared Savings Program ACO.
(2) Each ACO participant that submits claims for services used to determine the ACO's assigned population under subpart E of this part must be exclusive to one Shared Savings Program ACO. If, during a benchmark or performance year (including the 3-month claims runout for such benchmark or performance year), an ACO participant that participates in more than one ACO submits claims for services used in assignment under subpart E of this part, then:
(i) CMS will not consider any services billed through the TIN of the ACO participant when performing assignment under subpart E of this part for the benchmark or performance year.
[80 FR 32840, June 9, 2015, as amended at 82 FR 53369, Nov. 15, 2017]
§ 425.308 Public reporting and transparency.
(a) ACO public reporting Web page. Each ACO must create and maintain a dedicated Web page on which it publicly reports the information set forth in paragraph (b) of this section. The ACO must report the address of such Web page to CMS in a form and manner specified by CMS and must notify CMS of changes to the web address in the form and manner specified by CMS.
(b) Information to be reported. The ACO must publicly report the following information in a standardized format specified by CMS:
(1) Name and location.
(2) Primary contact.
(3) Organizational information, including all of the following:
(i) Identification of ACO participants.
(ii) Identification of participants in joint ventures between ACO professionals and hospitals.
(iii) Identification of the members of its governing body.
(iv) Identification of key clinical and administrative leadership.
(v) Identification of associated committees and committee leadership.
(vi) Identification of the types of ACO participants or combinations of ACO participants (as listed in § 425.102(a)) that formed the ACO.
(4) Shared savings and losses information, including the following:
(i) Amount of any payment of shared savings received by the ACO or shared losses owed to CMS.
(ii) Total proportion of shared savings invested in infrastructure, redesigned care processes and other resources required to support the three-part aim goals of better health for populations, better care for individuals and lower growth in expenditures, including the proportion distributed among ACO participants.
(5) The ACO's performance on all quality measures.
(6) Use of payment rule waivers under § 425.612, if applicable, or telehealth services under § 425.613, if applicable, or both.
(7) Information about a beneficiary incentive program established under § 425.304(c), if applicable, including the following, for each performance year:
(i) Total number of beneficiaries who received an incentive payment.
(ii) Total number of incentive payments furnished.
(iii) HCPCS codes associated with any qualifying service for which an incentive payment was furnished.
(iv) Total value of all incentive payments furnished.
(v) Total of each type of incentive payment (for example, check or debit card) furnished.
(c) Approval of public reporting information. Information reported on an ACO's public reporting Web page in compliance with the requirements of the standardized format specified by CMS is not subject to marketing review and approval under § 425.310.
(d) Public reporting by CMS. CMS may publicly report ACO-specific information, including but not limited to the ACO public reporting Web page address and the information required to be publicly reported under paragraph (b) of this section.
[80 FR 32840, June 9, 2015, as amended at 83 FR 68068, Dec. 31, 2018]
§ 425.310 Marketing requirements.
(a) File and use. Marketing materials and activities, as defined in § 425.20, may be used or conducted five business days following their submission to CMS if -
(1) The ACO certifies compliance with all the marketing requirements under this section; and
(2) CMS does not disapprove the marketing materials or activities.
(b) Deemed approval.
(1) Marketing materials and activities are deemed approved after expiration of the initial 5 day review period specified in paragraph (a) of this section.
(2)
(i) CMS may issue written notice of disapproval of marketing materials and activities at any time, including after the expiration of the initial 5 day review period.
(ii) The ACO, ACO participant, ACO provider/supplier, or another individual or entity performing functions or services related to ACO activities as applicable, must discontinue use of any marketing materials or activities disapproved by CMS.
(c) Marketing requirements. Marketing materials and activities must meet all of the following:
(1) Use template language developed by CMS, if available.
(2) Not be used in a discriminatory manner or for discriminatory purposes.
(3) Comply with § 425.304 regarding beneficiary incentives.
(4) Not be materially inaccurate or misleading.
(d) Sanctions. Failure to comply with this section will subject the ACO to the penalties set forth in § 425.216, termination under § 425.218, or both.
[76 FR 67973, Nov. 2, 2011, as amended at 83 FR 68068, Dec. 31, 2018]
§ 425.312 Beneficiary notifications.
(a) Notifications to fee-for-service beneficiaries.
(1) An ACO shall ensure that Medicare fee-for-service beneficiaries are notified about all of the following in the manner set forth in paragraph (a)(2) of this section:
(i) That each ACO participant and its ACO providers/suppliers are participating in the Shared Savings Program.
(ii) The beneficiary's opportunity to decline claims data sharing under § 425.708.
(iii) Beginning July 1, 2019, the beneficiary's ability to, and the process by which, he or she may identify or change identification of the individual he or she designated for purposes of voluntary alignment (as described in § 425.402(e)).
(2) Notification of the information specified in paragraph (a)(1) of this section must be carried out through the following methods:
(i) By an ACO participant posting signs in its facilities and, in settings in which beneficiaries receive primary care services, making standardized written notices available upon request.
(ii) During the performance year beginning on July 1, 2019 and each subsequent performance year, by an ACO or ACO participant providing each beneficiary with a standardized written notice prior to or at the first primary care visit of the performance year in the form and manner specified by CMS.
(b) Beneficiary incentive program notifications.
(1) Beginning July 1, 2019, an ACO that operates a beneficiary incentive program under § 425.304(c) shall ensure that the ACO or its ACO participants notify assigned beneficiaries of the availability of the beneficiary incentive program, including a description of the qualifying services for which an assigned beneficiary is eligible to receive an incentive payment (as described in § 425.304(c)).
(2) Notification of the information specified in paragraph (b)(1) of this section must be carried out by an ACO or ACO participant during each relevant performance year by providing each assigned beneficiary with a standardized written notice prior to or at the first primary care visit of the performance year in the form and manner specified by CMS.
(c) The beneficiary notifications under this section meet the definition of marketing materials and activities under § 425.20 and therefore must meet all applicable marketing requirements described in § 425.310.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32840, June 9, 2015; 83 FR 68068, Dec. 31, 2018]
§ 425.314 Audits and record retention.
(a) Right to audit. The ACO must agree, and must require its ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities to agree, that the CMS, DHHS, the Comptroller General, the Federal Government or their designees have the right to audit, inspect, investigate, and evaluate any books, contracts, records, documents and other evidence of the ACO, ACO participants, and ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities that pertain to all of the following:
(1) The ACO's compliance with Shared Savings Program.
(2) The quality of services performed and determination of amount due to or from CMS under the participation agreement.
(3) The ability of the ACO to bear the risk of potential losses and to repay any losses to CMS.
(4) The ACO's operation of a beneficiary incentive program.
(b) Maintenance of records. An ACO must agree, and must require its ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities to agree to the following:
(1) To maintain and give CMS, DHHS, the Comptroller General, the Federal Government or their designees access to all books, contracts, records, documents, and other evidence (including data related to Medicare utilization and costs, quality performance measures, shared savings distributions, information related to operation of a beneficiary incentive program, and other financial arrangements related to ACO activities) sufficient to enable the audit, evaluation, investigation, and inspection of the ACO's compliance with program requirements, quality of services performed, right to any shared savings payment, or obligation to repay losses, ability to bear the risk of potential losses, and ability to repay any losses to CMS.
(2) To maintain such books, contracts, records, documents, and other evidence for a period of 10 years from the final date of the agreement period or from the date of completion of any audit, evaluation, or inspection, whichever is later, unless—
(i) CMS determines there is a special need to retain a particular record or group of records for a longer period and notifies the ACO at least 30 days before the normal disposition date; or
(ii) There has been a termination, dispute, or allegation of fraud or similar fault against the ACO, its ACO participants, its ACO providers/suppliers, or other individuals or entities performing functions or services related to ACO activities, in which case ACOs must retain records for an additional 6 years from the date of any resulting final resolution of the termination, dispute, or allegation of fraud or similar fault.
(c) Responsibility of the ACO. Notwithstanding any arrangements between or among an ACO, ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to ACO activities, the ACO must have ultimate responsibility for adhering to and otherwise fully complying with all terms and conditions of its participation agreement with CMS, including the requirements set forth in this section.
(d) OIG authority. None of the provisions of this part limit or restrict OIG's authority to audit, evaluate, investigate, or inspect the ACO, its ACO participants, its ACO providers/suppliers and other individuals or entities performing functions or services related to ACO activities.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32840, June 9, 2015; 81 FR 38013, June 10, 2016; 83 FR 68068, Dec. 31, 2018]
§ 425.315 Reopening determinations of ACO shared savings or shared losses to correct financial reconciliation calculations.
(a) Reopenings.
(1) If CMS determines that the amount of shared savings due to the ACO or the amount of shared losses owed by the ACO has been calculated in error, CMS may reopen the initial determination or a final agency determination under subpart I of this part and issue a revised initial determination:
(i) At any time in the case of fraud or similar fault as defined in § 405.902; or
(ii) Not later than 4 years after the date of the notification to the ACO of the initial determination of savings or losses for the relevant performance year under § 425.604(f), § 425.605(e), § 425.606(h), § 425.609(e) or § 425.610(h), for good cause.
(2) Good cause may be established when—
(i) There is new and material evidence that was not available or known at the time of the payment determination and may result in a different conclusion; or
(ii) The evidence that was considered in making the payment determination clearly shows on its face that an obvious error was made at the time of the payment determination.
(3) A change of legal interpretation or policy by CMS in a regulation, CMS ruling or CMS general instruction, whether made in response to judicial precedent or otherwise, is not a basis for reopening a payment determination under this section.
(4) CMS has sole discretion to determine whether good cause exists for reopening a payment determination under this section.
(b) [Reserved]
[81 FR 38013, June 10, 2016, as amended at 83 FR 60092, Nov. 23, 2018; 83 FR 68068, Dec. 31, 2018]
§ 425.316 Monitoring of ACOs.
(a) General rule.
(1) In order to ensure that the ACO continues to satisfy the eligibility and program requirements under this part, CMS monitors and assesses the performance of ACOs, their ACO participants, and ACO providers/suppliers.
(2) CMS employs a range of methods to monitor and assess the performance of ACOs, ACO participants, and ACO providers/suppliers, including but not limited to any of the following, as appropriate:
(i) Analysis of specific financial and quality measurement data reported by the ACO as well as aggregate annual and quarterly reports.
(ii) Analysis of beneficiary and provider complaints.
(iii) Audits (including, for example, analysis of claims, chart review (medical record), beneficiary survey reviews, coding audits, on-site compliance reviews).
(b) Monitoring ACO avoidance of at-risk beneficiaries.
(1) CMS may use one or more of the methods described in paragraph (a)(2) of this section (as appropriate) to identify trends and patterns suggesting that an ACO has avoided at-risk beneficiaries. The results of these analyses may subsequently require further investigation and follow-up with beneficiaries or the ACO and its ACO participants, ACO providers/suppliers, or other individuals or entities performing functions or services related to the ACO's activities, in order to substantiate cases of beneficiary avoidance.
(2)
(i) CMS, at its sole discretion, may take any of the pre-termination actions set forth in § 425.216(a)(1) or immediately terminate, if it determines that an ACO, its ACO participants, any ACO providers/suppliers, or other individuals or entities performing functions or services related to the ACO's activities avoids at-risk beneficiaries.
(ii) If CMS requires the ACO to submit a CAP, the ACO will -
(A) Submit a CAP that addresses actions the ACO will take to ensure that the ACO, ACO participants, ACO providers/suppliers, or other individuals or entities performing functions or services related to the ACO's activities cease avoidance of at-risk beneficiaries.
(B) Not receive any shared savings payments during the time it is under the CAP.
(C) Not be eligible to receive shared savings for the performance year attributable to the time that necessitated the CAP (the time period during which the ACO avoided at risk beneficiaries).
(iii) CMS will re-evaluate the ACO during and after the CAP implementation period to determine if the ACO has continued to avoid at-risk beneficiaries. The ACO will be terminated if CMS determines that the ACO has continued to avoid at-risk beneficiaries during or after the CAP implementation period.
(c) Monitoring ACO compliance with quality performance standards. To identify ACOs that are not meeting the quality performance standards, CMS will review an ACO's submission of quality measurement data under § 425.500 or § 425.512. CMS may request additional documentation from an ACO, ACO participants, or ACO providers/suppliers, as appropriate. If an ACO does not meet quality performance standards or fails to report on one or more quality measures, CMS will take the following actions:
(1) For performance years (or a performance period) beginning on or before January 1, 2020.
(i) The ACO may be given a warning for the first time it fails to meet the minimum attainment level on at least 70 percent of the measures, as determined under § 425.502, in one or more domains and may be subject to a CAP. CMS may forgo the issuance of the warning letter depending on the nature and severity of the noncompliance and instead subject the ACO to actions set forth at § 425.216 or immediately terminate the ACO's participation agreement under § 425.218.
(ii) The ACO's compliance with the quality performance standards will be re-evaluated the following year. If the ACO continues to fail to meet the quality performance standard in the following year, the agreement will be terminated.
(iii) An ACO will not qualify to share in savings in any year it fails to report accurately, completely, and timely on the quality performance measures.
(2) For performance years beginning on or after January 1, 2021.
(i) If the ACO fails to meet the quality performance standard, CMS may take one or more of the actions prior to termination specified in § 425.216. Depending on the nature and severity of the noncompliance, CMS may forgo pre-termination actions and may immediately terminate the ACO's participation agreement under § 425.218.
(ii) CMS will terminate an ACO's participation agreement under any of the following circumstances:
(A) The ACO fails to meet the quality performance standard for 2 consecutive performance years within an agreement period.
(B) The ACO fails to meet the quality performance standard for any 3 performance years within an agreement period, regardless of whether the years are in consecutive order.
(C) A renewing ACO or re-entering ACO fails to meet the quality performance standard for the last performance year of the ACO's previous agreement period and this occurrence was either the second consecutive performance year of failed quality performance or the third nonconsecutive performance year of failed quality performance during the previous agreement period.
(D) A renewing ACO or re-entering ACO fails to meet the quality performance standard for 2 consecutive performance years across 2 agreement periods, specifically the last performance year of the ACO's previous agreement period and the first performance year of the ACO's new agreement period.
(d) Monitoring ACO financial performance.
(1) For performance years beginning on July 1, 2019 and subsequent performance years, CMS determines whether the Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries for the performance year exceed the ACO's updated benchmark by an amount equal to or exceeding either the ACO's negative MSR under a one-sided model, or the ACO's MLR under a two-sided model.
(2) If the Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries for the performance year exceed the ACO's updated benchmark as specified in paragraph (d)(1) of this section, CMS may take any of the pre-termination actions set forth in § 425.216.
(3) If the Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries for the performance year exceed the ACO's updated benchmark as specified in paragraph (d)(1) of this section for another performance year of the agreement period, CMS may immediately or with advance notice terminate the ACO's participation agreement under § 425.218.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32840, June 9, 2015; 81 FR 80559, Nov. 15, 2016; 83 FR 68069, Dec. 31, 2018; 85 FR 85039, Dec. 28, 2020]
Subpart E - Assignment of Beneficiaries
§ 425.400 General.
(a)
(1) General. CMS employs the assignment methodology described in § 425.402 and § 425.404 for purposes of benchmarking, preliminary prospective assignment (including quarterly updates), retrospective reconciliation, and prospective assignment.
(i) A Medicare fee-for-service beneficiary is assigned to an ACO if the -
(A) Beneficiary meets the eligibility criteria under § 425.401(a); and
(ii) CMS applies a step-wise process based on the beneficiary's utilization of primary care services provided under Title XVIII by a physician who is an ACO professional during each performance year for which shared savings are to be determined and, with respect to ACOs participating in a 6-month performance year during CY 2019, during the entirety of CY 2019 as specified in § 425.609.
(2) Preliminary prospective assignment with retrospective reconciliation.
(i) Medicare assigns beneficiaries in a preliminary manner at the beginning of a performance year based on most recent data available.
(ii) Assignment will be updated quarterly based on the most recent 12 months of data.
(iii) In determining final assignment for a benchmark or performance year, CMS will exclude any services furnished during the benchmark or performance year that are billed through the TIN of an ACO participant that is an ACO participant in more than one ACO.
(3) Prospective assignment.
(i) Medicare fee-for-service beneficiaries are prospectively assigned to an ACO at the beginning of each benchmark or performance year based on the beneficiary's use of primary care services in the most recent 12 months for which data are available, using the assignment methodology described in §§ 425.402 and 425.404.
(ii) Beneficiaries that are prospectively assigned to an ACO under paragraph (a)(3)(i) of this section will remain assigned to the ACO at the end of the benchmark or performance year unless they meet any of the exclusion criteria under § 425.401(b).
(4) Assignment methodology applied to ACO.
(i) For agreement periods beginning before July 1, 2019, the applicable assignment methodology is determined based on track as specified in § 425.600(a).
(A) Preliminary prospective assignment with retrospective reconciliation as described in paragraph (a)(2) of this section applies to Track 1 and Track 2 ACOs.
(B) Prospective assignment as described in paragraph (a)(3) of this section applies to Track 3 ACOs.
(ii) For agreement periods beginning on July 1, 2019 and in subsequent years, an ACO may select the assignment methodology that CMS employs for assignment of beneficiaries under this subpart.
(A) An ACO may select either of the following:
(1) Preliminary prospective assignment with retrospective reconciliation, as described in paragraph (a)(2) of this section.
(2) Prospective assignment, as described in paragraph (a)(3) of this section.
(B) This selection is made prior to the start of each agreement period, and may be modified prior to the start of each performance year as specified in § 425.226.
(b) Beneficiary assignment to an ACO is for purposes of determining the population of Medicare fee-for-service beneficiaries for whose care the ACO is accountable under subpart F of this part, and for determining whether an ACO has achieved savings under subpart G of this part, and in no way diminishes or restricts the rights of beneficiaries assigned to an ACO to exercise free choice in determining where to receive health care services.
(c) Primary care services for purposes of assigning beneficiaries are identified by selected HCPCS/CPT codes, or revenue center codes.
(1) Primary care service codes are as follows:
(i) For performance years 2012 through 2015:
(A) CPT codes:
(1) 99201 through 99215.
(2) 99304 through 99340.
(3) 99341 through 99350.
(B) HCPCS codes G0402 (the code for the Welcome to Medicare visit) and G0438 and G0439 (codes for the annual wellness visits).
(C) Revenue center codes 0521, 0522, 0524, and 0525 submitted by FQHCs (for services furnished prior to January 1, 2011), or by RHCs.
(ii) For performance year 2016 as follows:
(A) CPT codes:
(1) 99201 through 99215.
(2) 99304 through 99340.
(3) 99341 through 99350.
(4) 99495, 99496, and 99490.
(B) HCPCS codes:
(1) G0402 (the code for the Welcome to Medicare visit) and
(2) G0438 and G0439 (codes for the annual wellness visits).
(3) G0463 for services furnished in ETA hospitals.
(C) Revenue center codes 0521, 0522, 0524, and 0525 submitted by FQHCs (for services furnished prior to January 1, 2011), or by RHCs.
(iii) For performance years 2017 and 2018 as follows:
(A) CPT codes:
(1) 99201 through 99215.
(2) 99304 through 99318 (excluding claims including the POS 31 modifier).
(3) 99319 through 99340.
(4) 99341 through 99350.
(5) 99495, 99496, and 99490.
(B) HCPCS Codes:
(1) G0402 (the code for the Welcome to Medicare visit) and
(2) G0438 and G0439 (codes for the annual wellness visits).
(3) G0463 for services furnished in ETA hospitals.
(C) Revenue center codes 0521, 0522, 0524, and 0525 submitted by FQHCs (for services furnished prior to January 1, 2011), or by RHCs.
(iv) For performance years (or a performance period) during 2019, and performance year 2020 as follows:
(A) CPT codes:
(1) 99201 through 99215 (codes for office or other outpatient visit for the evaluation and management of a patient).
(2) 99304 through 99318 (codes for professional services furnished in a nursing facility; services identified by these codes furnished in a SNF are excluded).
(3) 99319 through 99340 (codes for patient domiciliary, rest home, or custodial care visit).
(4) 99341 through 99350 (codes for evaluation and management services furnished in a patients' home for claims identified by place of service modifier 12).
(5) 99487, 99489 and 99490 (codes for chronic care management).
(6) 99495 and 99496 (codes for transitional care management services).
(7) 99497 and 99498 (codes for advance care planning).
(8) 96160 and 96161 (codes for administration of health risk assessment).
(9) 99354 and 99355 (add-on codes, for prolonged evaluation and management or psychotherapy services beyond the typical service time of the primary procedure; when the base code is also a primary care service code under this paragraph (c)(1)).
(10) 99484, 99492, 99493 and 99494 (codes for behavioral health integration services).
(B) HCPCS codes:
(1) G0402 (the code for the Welcome to Medicare visit) and
(2) G0438 and G0439 (codes for the annual wellness visits).
(3) G0463 for services furnished in ETA hospitals.
(4) G0506 (code for chronic care management).
(5) G0444 (codes for annual depression screening service).
(6) G0442 (code for alcohol misuse screening service).
(7) G0443 (code for alcohol misuse counseling service).
(v) For the performance year starting on January 1, 2021, and subsequent performance years as follows:
(A) CPT codes:
(1) 96160 and 96161 (codes for administration of health risk assessment).
(2) 99201 through 99215 (codes for office or other outpatient visit for the evaluation and management of a patient).
(3) 99304 through 99318 (codes for professional services furnished in a nursing facility; professional services or services reported on an FQHC or RHC claim identified by these codes are excluded when furnished in a SNF).
(4) 99319 through 99340 (codes for patient domiciliary, rest home, or custodial care visit).
(5) 99341 through 99350 (codes for evaluation and management services furnished in a patient's home for claims identified by place of service modifier 12).
(6) 99354 and 99355 (add-on codes, for prolonged evaluation and management or psychotherapy services beyond the typical service time of the primary procedure; when the base code is also a primary care service code under this paragraph (c)(1)(v)).
(7) 99421, 99422, and 99423 (codes for online digital evaluation and management).
(8) 99439 (code for non-complex chronic care management).
(9) 99483 (code for assessment of and care planning for patients with cognitive impairment).
(10) 99484, 99492, 99493 and 99494 (codes for behavioral health integration services).
(11) 99487, 99489, 99490 and 99491 (codes for chronic care management).
(12) 99495 and 99496 (codes for transitional care management services).
(13) 99497 and 99498 (codes for advance care planning; services identified by these codes furnished in an inpatient setting are excluded).
(B) HCPCS codes:
(1) G0402 (code for the Welcome to Medicare visit).
(2) G0438 and G0439 (codes for the annual wellness visits).
(3) G0442 (code for alcohol misuse screening service).
(4) G0443 (code for alcohol misuse counseling service).
(5) G0444 (code for annual depression screening service).
(6) G0463 (code for services furnished in ETA hospitals).
(7) G0506 (code for chronic care management).
(8) G2010 (code for the remote evaluation of patient video/images).
(9) G2012 (code for virtual check-in).
(10) G2058 (code for non-complex chronic care management).
(11) G2064 and G2065 (codes for principal care management services).
(12) G2214 (code for psychiatric collaborative care model).
(2)
(i) When the assignment window (as defined in § 425.20) for a benchmark or performance year includes any month(s) during the COVID-19 Public Health Emergency defined in § 400.200 of this chapter, in determining beneficiary assignment, we use the primary care service codes identified in paragraph (c)(1) of this section, and additional primary care service codes as follows:
(A) CPT codes:
(1) 99421, 99422, and 99423 (codes for online digital evaluation and management services).
(2) 99441, 99442, and 99443 (codes for telephone evaluation and management services).
(B) HCPCS codes:
(1) G2010 (code for the remote evaluation of patient video/images).
(2) G2012 (code for virtual check-in).
(ii) The additional primary care service codes specified in paragraph (c)(2)(i) of this section are applicable to all months of the assignment window (as defined in § 425.20), when the assignment window includes any month(s) during the COVID-19 Public Health Emergency defined in § 400.200 of this chapter.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32840, June 9, 2015; 82 FR 53369, Nov. 15, 2017; 83 FR 60092, Nov. 23, 2018; 83 FR 68069, Dec. 31, 2018; 85 FR 27625, May 8, 2020; 85 FR 85040, Dec. 28, 2020]
§ 425.401 Criteria for a beneficiary to be assigned to an ACO.
(a) A beneficiary may be assigned to an ACO under the assignment methodology in §§ 425.402 and 425.404, for a performance or benchmark year, if the beneficiary meets all of the following criteria during the assignment window:
(1)
(i) Has at least 1 month of Part A and Part B enrollment; and
(ii) Does not have any months of Part A only or Part B only enrollment.
(2) Does not have any months of Medicare group (private) health plan enrollment.
(3) Is not assigned to any other Medicare shared savings initiative.
(4) Lives in the United States or U.S. territories and possessions, based on the most recent available data in our beneficiary records regarding the beneficiary's residence at the end of the assignment window.
(b) A beneficiary is excluded from the prospective assignment list of an ACO that is participating under prospective assignment under § 425.400(a)(3) at the end of a performance or benchmark year and quarterly during each performance year consistent with § 425.400(a)(3)(ii), or at the end of CY 2019 as specified in § 425.609(b)(1)(ii) and (c)(1)(ii) if the beneficiary meets any of the following criteria during the performance or benchmark year:
(1)
(i) Does not have at least 1 month of Part A and Part B enrollment; and
(ii) Has any months of Part A only or Part B only enrollment.
(2) Has any months of Medicare group (private) health plan enrollment.
(3) Did not live in the United States or U.S. territories and possessions, based on the most recent available data in our beneficiary records regarding the beneficiary's residency at the end of the year.
[80 FR 32840, June 9, 2015, as amended at 83 FR 60093, Nov. 23, 2018; 83 FR 68069, Dec. 31, 2018]
§ 425.402 Basic assignment methodology.
(a) For performance years 2012 through 2015, CMS employs the following step-wise methodology to assign Medicare beneficiaries to an ACO after identifying all patients that had at least one primary care service with a physician who is an ACO professional of that ACO:
(1)
(i) Identify all primary care services rendered by primary care physicians during one of the following:
(A) The most recent 12 months (for purposes of preliminary prospective assignment and quarterly updates to the preliminary prospective assignment).
(B) The performance year (for purposes of final assignment).
(ii) The beneficiary is assigned to an ACO if the allowed charges for primary care services furnished to the beneficiary by all the primary care physicians who are ACO professionals in the ACO are greater than the allowed charges for primary care services furnished by primary care physicians who are -
(A) ACO professionals in any other ACO; and
(B) Not affiliated with any ACO and identified by a Medicare-enrolled TIN.
(2) The second step considers the remainder of the beneficiaries who have received at least one primary care service from an ACO physician, but who have not had a primary care service rendered by any primary care physician, either inside or outside the ACO. The beneficiary will be assigned to an ACO if the allowed charges for primary care services furnished to the beneficiary by all ACO professionals in the ACO are greater than the allowed charges for primary care services furnished by -
(i) All ACO professionals in any other ACO; and
(ii) Other physicians, nurse practitioners, physician assistants, clinical nurse specialists who are unaffiliated with an ACO and are identified by a Medicare-enrolled TIN.
(b) For performance year 2016 and subsequent performance years, CMS employs the following step-wise methodology to assign Medicare fee-for-service beneficiaries to an ACO based on available claims information:
(1) Identify all beneficiaries that had at least one primary care service with a physician who is an ACO professional in the ACO and who is a primary care physician as defined under § 425.20 or who has one of the primary specialty designations included in paragraph (c) of this section.
(2) Identify all primary care services furnished to beneficiaries identified in paragraph (b)(1) of this section by ACO professionals of that ACO who are primary care physicians as defined under § 425.20, non-physician ACO professionals, and physicians with specialty designations included in paragraph (c) of this section during the applicable assignment window.
(3) Under the first step, a beneficiary identified in paragraph (b)(1) of this section is assigned to an ACO if the allowed charges for primary care services furnished to the beneficiary by primary care physicians who are ACO professionals and non-physician ACO professionals in the ACO are greater than the allowed charges for primary care services furnished by primary care physicians, nurse practitioners, physician assistants, and clinical nurse specialists who are -
(i) ACO professionals in any other ACO; or
(ii) Not affiliated with any ACO and identified by a Medicare-enrolled billing TIN.
(4) The second step considers the remainder of the beneficiaries identified in paragraph (b)(1) of this section who have not had a primary care service rendered by any primary care physician, nurse practitioner, physician assistant, or clinical nurse specialist, either inside the ACO or outside the ACO. The beneficiary will be assigned to an ACO if the allowed charges for primary care services furnished to the beneficiary by physicians who are ACO professionals with specialty designations as specified in paragraph (c) of this section are greater than the allowed charges for primary care services furnished by physicians with specialty designations as specified in paragraph (c) of this section -
(i) Who are ACO professionals in any other ACO; or
(ii) Who are unaffiliated with an ACO and are identified by a Medicare-enrolled billing TIN.
(c) ACO professionals considered in the second step of the assignment methodology in paragraph (b)(4) of this section include physicians who have one of the following primary specialty designations:
(1) Cardiology.
(2) Osteopathic manipulative medicine.
(3) Neurology.
(4) Obstetrics/gynecology.
(5) Sports medicine.
(6) Physical medicine and rehabilitation.
(7) Psychiatry.
(8) Geriatric psychiatry.
(9) Pulmonary disease.
(10) Nephrology.
(11) Endocrinology.
(12) Multispecialty clinic or group practice.
(13) Addiction medicine.
(14) Hematology.
(15) Hematology/oncology.
(16) Preventive medicine.
(17) Neuropsychiatry.
(18) Medical oncology.
(19) Gynecology/oncology.
(d) When considering services furnished by ACO professionals in teaching hospitals that have elected under § 415.160 of this subchapter to receive payment on a reasonable cost basis for the direct medical and surgical services of their physicians in the assignment methodology under paragraph (b) of this section, CMS uses an estimated amount based on the amounts payable under the physician fee schedule for similar services in the geographic location of the teaching hospital as a proxy for the amount of the allowed charges for the service.
(e) For performance year 2018 and subsequent performance years, if a system is available to allow a beneficiary to designate a provider or supplier as responsible for coordinating their overall care and for CMS to process the designation electronically, CMS will supplement the claims-based assignment methodology described in this section with information provided by beneficiaries regarding the provider or supplier they consider responsible for coordinating their overall care. Such designations must be made in the form and manner and by a deadline determined by CMS.
(1) Notwithstanding the assignment methodology under paragraph (b) of this section, beneficiaries who designate an ACO professional participating in an ACO as responsible for coordinating their overall care are prospectively assigned to that ACO, regardless of track, annually at the beginning of each benchmark and performance year based on available data at the time assignment lists are determined for the benchmark and performance year.
(2) Beneficiaries are added to the ACO's list of assigned beneficiaries if all of the following conditions are satisfied:
(i) For performance year 2018:
(A) The beneficiary must have had at least one primary care service during the assignment window as defined under § 425.20 with a physician who is an ACO professional in the ACO who is a primary care physician as defined under § 425.20 or who has one of the primary specialty designations included in paragraph (c) of this section.
(B) The beneficiary meets the eligibility criteria established at § 425.401(a) and must not be excluded by the criteria at § 425.401(b). The exclusion criteria at § 425.401(b) apply for purposes of determining beneficiary eligibility for alignment to ACOs under all tracks based on the beneficiary's designation of an ACO professional as responsible for coordinating their overall care under paragraph (e) of this section.
(C) The beneficiary must have designated an ACO professional who is a primary care physician as defined at § 425.20, a physician with a specialty designation included at paragraph (c) of this section, or a nurse practitioner, physician assistant, or clinical nurse specialist as responsible for coordinating their overall care.
(D) If a beneficiary has designated a provider or supplier outside the ACO who is a primary care physician as defined at § 425.20, a physician with a specialty designation included at paragraph (c) of this section, or a nurse practitioner, physician assistant, or clinical nurse specialist, as responsible for coordinating their overall care, the beneficiary is not added to the ACO's list of assigned beneficiaries under the assignment methodology in paragraph (b) of this section.
(ii) For performance years starting on January 1, 2019, and subsequent performance years:
(A) The beneficiary meets the eligibility criteria established at § 425.401(a) and must not be excluded by the criteria at § 425.401(b). The exclusion criteria at § 425.401(b) apply for purposes of determining beneficiary eligibility for alignment to an ACO based on the beneficiary's designation of an ACO professional as responsible for coordinating their overall care under paragraph (e) of this section, regardless of the ACO's assignment methodology selection under § 425.400(a)(4)(ii).
(B) The beneficiary must have designated an ACO professional as responsible for coordinating their overall care.
(C) If a beneficiary has designated a provider or supplier outside the ACO as responsible for coordinating their overall care, the beneficiary is not added under the assignment methodology in paragraph (b) of this section to the ACO's list of assigned beneficiaries for a 12-month performance year or the ACO's list of assigned beneficiaries for a 6-month performance year, which is based on the entire CY 2019 as provided in § 425.609.
(D) The beneficiary is not assigned to an entity participating in a model tested or expanded under section 1115A of the Act under which claims-based assignment is based solely on claims for services other than primary care services and for which there has been a determination by the Secretary that waiver of the requirement in section 1899(c)(2)(B) of the Act is necessary solely for purposes of testing the model.
(3) The ACO, ACO participants, ACO providers/suppliers, ACO professionals, and other individuals or entities performing functions and services related to ACO activities are prohibited from providing or offering gifts or other remuneration to Medicare beneficiaries as inducements for influencing a Medicare beneficiary's decision to designate or not to designate an ACO professional under paragraph (e) of this section. The ACO, ACO participants, ACO providers/suppliers, ACO professionals, and other individuals or entities performing functions and services related to ACO activities must not, directly or indirectly, commit any act or omission, nor adopt any policy that coerces or otherwise influences a Medicare beneficiary's decision to designate or not to designate an ACO professional as responsible for coordinating their overall care under paragraph (e) of this section, including but not limited to the following:
(i) Offering anything of value to the Medicare beneficiary as an inducement to influence the Medicare beneficiary's decision to designate or not to designate an ACO professional as responsible for coordinating their overall care under paragraph (e) of this section. Any items or services provided in violation of paragraph (e)(3) of this section are not considered to have a reasonable connection to the medical care of the beneficiary, as required under § 425.304(b)(1).
(ii) Withholding or threatening to withhold medical services or limiting or threatening to limit access to care.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32841, June 9, 2015; 80 FR 71386, Nov. 16, 2015; 81 FR 80559, Nov. 15, 2016; 83 FR 60093, Nov. 23, 2018; 83 FR 68069, Dec. 31, 2018]
§ 425.404 Special assignment conditions for ACOs including FQHCs and RHCs.
CMS assigns beneficiaries to ACOs based on services furnished in FQHCs or RHCs or both consistent with the general assignment methodology in § 425.402, with special conditions:
(a) For performance years 2012 through 2018—
(1) Such ACOs are required to identify, through an attestation, physicians who directly provide primary care services in each FQHC or RHC that is an ACO participant and/or ACO provider/supplier in the ACO.
(2) Under the assignment methodology in § 425.402, CMS treats a service reported on an FQHC/RHC claim as a primary care service—
(i) If the claim includes a HCPCS or revenue center code that meets the definition of primary care services under § 425.20;
(ii) Performed by a primary care physician if the NPI of a physician identified in the attestation provided under paragraph (a)(1) of this section is reported on the claim for a primary care service (as described in paragraph (a)(2)(i) of this section) as the attending provider; and
(iii) Performed by a non-physician ACO professional if the NPI reported on the claim for a primary care service (as described in paragraph (a)(2)(i) of this section) as the attending provider is an ACO professional but is not identified in the attestation provided under paragraph (a)(1) of this section.
(b) For performance years starting on January 1, 2019, and subsequent performance years, under the assignment methodology in § 425.402, CMS treats a service reported on an FQHC/RHC claim as a primary care service performed by a primary care physician.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32841, June 9, 2015; 82 FR 53369, Nov. 15, 2017; 83 FR 60093, Nov. 23, 2018]
Subpart F - Quality Performance Standards and Reporting
§ 425.500 Measures to assess the quality of care furnished by an ACO for performance years (or a performance period) beginning on or before January 1, 2020.
(a) General. CMS establishes quality performance measures to assess the quality of care furnished by the ACO. If the ACO demonstrates to CMS that it has satisfied the quality performance requirements in this subpart, and the ACO meets all other applicable requirements, the ACO is eligible for shared savings.
(b) Selecting measures.
(1) CMS selects the measures designated to determine an ACO's success in promoting the aims of better care for individuals, better health for populations, and lower growth in expenditures.
(2) CMS designates the measures for use in the calculation of the quality performance standard.
(3) CMS seeks to improve the quality of care furnished by ACOs over time by specifying higher standards, new measures, or both.
(c) ACOs must submit data on the measures determined under paragraph (b) of this section according to the method of submission established by CMS.
(d) Patient experience of care survey.
(1) For performance years (or a performance period) beginning in 2014 through 2019, ACOs must select a CMS-certified vendor to administer the survey and report the results accordingly.
(2) For performance year 2020, CMS waives the CAHPS for ACOs reporting requirement and will assign all ACOs automatic credit for the CAHPS for ACOs survey measures.
(e) Audit and validation of data. CMS retains the right to audit and validate quality data reported by an ACO.
(1) In an audit, the ACO will provide beneficiary medical records data if requested by CMS.
(2) If, at the conclusion of the audit process the overall audit match rate between the quality data reported and the medical records provided under paragraph (e)(1) of this section is less than 80 percent, absent unusual circumstances, CMS will adjust the ACO's overall quality score proportional to the ACO's audit performance.
(3) If, at the conclusion of the audit process CMS determines there is an audit match rate of less than 90 percent, the ACO may be required to submit a CAP under § 425.216 for CMS approval.
(f) Failure to report quality measure data accurately, completely, and timely (or to timely correct such data) may subject the ACO to termination or other sanctions, as described in §§ 425.216 and 425.218.
[76 FR 67973, Nov. 2, 2011, as amended at 81 FR 80559, Nov. 15, 2016; 82 FR 53370, Nov. 15, 2017; 85 FR 85040, Dec. 28, 2020]
§ 425.502 Calculating the ACO quality performance score for performance years (or a performance period) beginning on or before January 1, 2020.
(a) Establishing a quality performance standard. CMS designates the quality performance standard in each performance year. The quality performance standard is the overall standard the ACO must meet in order to be eligible for shared savings.
(1) For the first performance year of an ACO's first agreement period, CMS defines the quality performance standard at the level of complete and accurate reporting for all quality measures.
(2) During subsequent performance years of the ACO's first agreement period, the quality performance standard will be phased in such that the ACO must continue to report all measures but the ACO will be assessed on performance based on the quality performance benchmark and minimum attainment level of all measures.
(3) Under the quality performance standard for each performance year of an ACO's subsequent agreement period, the ACO must continue to report on all measures but the ACO will be assessed on performance based on the quality performance benchmark and minimum attainment level of all measures.
(4) A newly introduced measure is set at the level of complete and accurate reporting for the first two reporting periods, the measure is required. For subsequent reporting periods, the quality performance standard for the measure will be assessed according to the phase-in schedule for the measure.
(5) CMS reserves the right to redesignate a measure as pay for reporting when the measure owner determines the measure no longer aligns with clinical practice or causes patient harm, or when there is a determination under the Quality Payment Program that the measure has undergone a substantive change.
(b) Establishing a performance benchmark and minimum attainment level for measures.
(1) CMS designates a performance benchmark and minimum attainment level for each measure, and establishes a point scale for the measures.
(2)
(i) CMS will define the quality benchmarks using fee-for-service Medicare data.
(ii) CMS will set benchmarks using flat percentages when the 60th percentile is equal to or greater than 80.00 percent, or when the 90th percentile is equal to or greater than 95 percent.
(iii) CMS reserves the right to use flat percentages for other measures when CMS determines that fee-for-service Medicare data are unavailable, inadequate, or unreliable to set the quality benchmarks.
(3) The minimum attainment level for pay for performance measures is set at 30 percent or the 30th percentile of the performance benchmark. The minimum attainment level for pay for reporting measures is set at the level of complete and accurate reporting.
(4)
(i) CMS will update the quality performance benchmarks every 2 years.
(ii) For newly introduced measures that transition to pay for performance in the second year of the 2-year benchmarking cycle, the benchmark will be established for that year and updated along with the other measures at the start of the next 2-year benchmarking cycle.
(iii) CMS will use up to three years of data, as available, to set the benchmark for each quality measure.
(c) Methodology for calculating a performance score for each measure.
(1) Performance below the minimum attainment level for a measure will receive zero points for that measure.
(2) Performance equal to or greater than the minimum attainment level for a pay-for-performance measure will receive points on a sliding scale based on the level of performance.
(3) Those measures designated as all or nothing measures will receive the maximum available points if all criteria are met and zero points if one or more of the criteria are not met.
(4) Performance at or above 90 percent or the 90th percentile of the performance benchmark earns the maximum points available for the measure.
(5) Performance equal to or greater than the minimum attainment level for pay-for-reporting measures will receive the maximum available points.
(d) Establishing quality requirements for domains.
(1) CMS groups individual measures into four domains:
(i) Patient/care giver experience.
(ii) Care coordination/Patient safety.
(iii) Preventative health.
(iv) At-risk population.
(2) To satisfy quality requirements for a domain:
(i) The ACO must report all measures within a domain.
(ii) CMS may take the compliance actions described in § 425.216 for ACOs exhibiting poor performance on a domain, as determined by CMS under § 425.316.
(iii)
(A) If the ACO achieves the minimum attainment level for at least one measure in each of the four domains, and also satisfies the requirements for realizing shared savings under subpart G of this part, the ACO may receive the proportion of those shared savings for which it qualifies.
(B) If an ACO fails to achieve the minimum attainment level on all measures in a domain, it will not be eligible to share in any savings generated.
(e) Methodology for calculating the ACO's overall performance score.
(1) CMS scores individual measures and determines the corresponding number of points that may be earned based on the ACO's performance.
(2) CMS adds the points earned for the individual measures within the domain and divides by the total points available for the domain to determine the domain score.
(3) Domains are weighted equally and scores averaged to determine the ACO's overall performance score and sharing rate.
(4)
(i) ACOs that demonstrate quality improvement on established quality measures from year to year will be eligible for up to 4 bonus points per domain.
(ii) Bonus points are awarded based on an ACO's net improvement in measures within a domain, which is calculated by determining the total number of significantly improved measures and subtracting the total number of significantly declined measures.
(iii) Up to four bonus points are awarded based on a comparison of the ACO's net improvement in performance on the measures for the domain to the total number of individual measures in the domain.
(iv) When bonus points are added to points earned for the quality measures in the domain, the total points received for the domain may not exceed the maximum total points for the domain in the absence of the quality improvement measure.
(v) If an ACO renews its participation agreement for a subsequent agreement period, quality improvement will be measured based on a comparison between performance in the first year of the new agreement period and performance in the last year of the previous agreement period.
(vi) For performance year 2017 and subsequent performance years, if an ACO receives the mean Shared Savings Program ACO quality score based on the extreme and uncontrollable circumstances policies in paragraph (f) of this section, the ACO is not eligible for bonus points awarded based on quality improvement.
(vii) For performance year 2017 and subsequent performance years, if an ACO receives the mean Shared Savings Program ACO quality score under paragraph (f) of this section, in the next performance year for which the ACO receives a quality performance score based on its own quality reporting, quality improvement is measured based on a comparison between the performance in that year and the most recently available prior performance year in which the ACO reported quality.
(f) Extreme and uncontrollable circumstances. For performance year 2017 and subsequent performance years, including the applicable quality data reporting period for the performance year, CMS uses an alternative approach to calculating the quality score for ACOs affected by extreme and uncontrollable circumstances instead of the methodology specified in paragraphs (a) through (e) of this section as follows:
(1) CMS determines the ACO was affected by an extreme and uncontrollable circumstance based on either of the following:
(i) Twenty percent or more of the ACO's assigned beneficiaries reside in an area identified under the Quality Payment Program as being affected by an extreme and uncontrollable circumstance.
(A) Assignment is determined under subpart E of this part.
(B) In making this determination for performance year 2017, CMS uses the final list of beneficiaries assigned to the ACO for the performance year. For performance year 2018 and subsequent performance years, CMS uses the list of assigned beneficiaries used to generate the Web Interface quality reporting sample.
(ii) The ACO's legal entity is located in an area identified under the Quality Payment Program as being affected by an extreme and uncontrollable circumstance. An ACO's legal entity location is based on the address on file for the ACO in CMS' ACO application and management system.
(2) If CMS determines the ACO meets the requirements of paragraph (f)(1) of this section, CMS calculates the ACO's quality score as follows:
(i) The ACO's minimum quality performance score is set to equal the mean quality performance score for all Shared Savings Program ACOs for the relevant performance year.
(ii) If the ACO completely and accurately reports all quality measures, CMS uses the higher of the ACO's quality performance score or the mean quality performance score for all Shared Savings Program ACOs.
(3) CMS applies determinations made under the Quality Payment Program with respect to—
(i) Whether an extreme and uncontrollable circumstance has occurred; and
(ii) The affected areas.
(4) CMS has sole discretion to determine the time period during which an extreme and uncontrollable circumstance occurred, the percentage of the ACO's assigned beneficiaries residing in the affected areas, and the location of the ACO legal entity.
[76 FR 67973, Nov. 2, 2011, as amended at 78 FR 74823, Dec. 10, 2013; 79 FR 68008, Nov. 13, 2014; 80 FR 71386, Nov. 16, 2015; 81 FR 80560, Nov. 15, 2016; 82 FR 53370, Nov. 15, 2017; 82 FR 60918, Dec. 26, 2017; 83 FR 60093, Nov. 23, 2018; 83 FR 68069, Dec. 31, 2018; 85 FR 19291, Apr. 6, 2020; 85 FR 85040, Dec. 28, 2020]
§ 425.504 Incorporating reporting requirements related to the Physician Quality Reporting System Incentive and Payment Adjustment.
(a) Physician quality reporting system.
(1) ACOs, on behalf of eligible professionals who bill under the TIN of an ACO participant, must submit the measures determined under § 425.500 using a CMS web interface, to qualify on behalf of their eligible professionals for the Physician Quality Reporting System incentive under the Shared Savings Program.
(2)
(i) Eligible professionals who bill under the TIN of an ACO participant within an ACO may only participate under their ACO participant TIN as a group practice under the Physician Quality Reporting System Group Practice Reporting Option of the Shared Savings Program for purposes of receiving an incentive payment under the Physician Quality Reporting System.
(ii) Under the Shared Savings Program, an ACO, on behalf of eligible professionals who bill under the TIN of an ACO participant must satisfactorily report the measures determined under Subpart F of this part during the reporting period according to the method of submission established by CMS under the Shared Savings Program in order to receive a Physician Quality Reporting System incentive under the Shared Savings Program.
(3) If eligible professionals who bill under the TIN of an ACO participant within an ACO qualify for a Physician Quality Reporting System incentive payment, each ACO participant TIN, on behalf of its ACO supplier/provider participants who are eligible professionals, will receive an incentive, for those years an incentive is available, based on the allowed charges under the Physician Fee Schedule for that TIN.
(4) ACO participant TINs and individual eligible professionals who bill under the TIN of an ACO participant cannot earn a Physician Quality Reporting System incentive outside of the Medicare Shared Savings Program.
(5) The Physician Quality Reporting System incentive under the Medicare Shared Savings Program is equal to 0.5 percent of the Secretary's estimate of the ACO's eligible professionals' total Medicare Part B Physician Fee Schedule allowed charges for covered professional services furnished during the calendar year reporting period from January 1 through December 31, for years 2012 through 2014.
(b) Physician Quality Reporting System payment adjustment for 2015.
(1) ACOs, on behalf of eligible professionals who bill under the TIN of an ACO participant, must submit one of the ACO GPRO measures determined under § 425.500 using a CMS web interface, to satisfactorily report on behalf of their eligible professionals for purposes of the 2015 Physician Quality Reporting System payment adjustment under the Shared Savings Program.
(2)
(i) Eligible professionals who bill under the TIN of an ACO participant within an ACO may only participate under their ACO participant TIN as a group practice under the Physician Quality Reporting System Group Practice Reporting Option of the Shared Savings Program for purposes of the 2015 Physician Quality Reporting System payment adjustment under the Shared Savings Program.
(ii) Under the Shared Savings Program, an ACO, on behalf of eligible professionals who bill under the TIN of an ACO participant, must satisfactorily report one of the measures determined under Subpart F of this part during the reporting period for a year, as defined in paragraph (b)(6) of this section, according to the method of submission established by CMS under the Shared Savings Program for purposes of the 2015 Physician Quality Reporting System payment adjustment.
(3) If an ACO, on behalf of eligible professionals who bill under the TIN of an ACO participant, does not satisfactorily report for purposes of a 2015 Physician Quality Reporting System payment adjustment, each eligible professional who bills under the TIN of an ACO participant, will receive a payment adjustment, as described in paragraph (b)(5) of this section.
(4) ACO participant TINs and individual eligible professionals who bill under the TIN of an ACO participant cannot satisfactorily report for purposes of a 2015 Physician Quality Reporting System payment adjustment outside of the Medicare Shared Savings Program.
(5) For eligible professionals subject to the 2015 Physician Quality Reporting System payment adjustment under the Medicare Shared Savings Program, the Medicare Part B Physician Fee Schedule amount for covered professional services furnished during the program year is equal to the applicable percent of the Medicare Part B Physician Fee Schedule amount that would otherwise apply to such services under section 1848 of the Act.
(i) The applicable percent for 2015 is 98.5 percent.
(ii) The applicable percent for 2016 and subsequent years is 98.0 percent.
(6) The reporting period for a year is the calendar year from January 1 through December 31 that occurs 2 years prior to the program year in which the payment adjustment is applied.
(c) Physician Quality Reporting System payment adjustment for 2016.
(1) ACOs, on behalf of eligible professionals who bill under the TIN of an ACO participant, must submit all of the ACO GPRO measures determined under § 425.500 using a CMS web interface, to satisfactorily report on behalf of their eligible professionals for purposes of the Physician Quality Reporting System payment adjustment under the Shared Savings Program for 2016.
(2) Eligible professionals who bill under the TIN of an ACO participant within an ACO may only participate under their ACO participant TIN as a group practice under the Physician Quality Reporting System Group Practice Reporting Option of the Shared Savings Program for purposes of the Physician Quality Reporting System payment adjustment under the Shared Savings Program for 2016 and subsequent years.
(3) If an ACO, on behalf of eligible professionals who bill under the TIN of an ACO participant, does not satisfactorily report for purposes of the Physician Quality Reporting System payment adjustment for 2016 and subsequent years, each eligible professional who bills under the TIN of an ACO participant, will receive a payment adjustment, as described in § 414.90(e) of this chapter.
(4) For eligible professionals subject to the Physician Quality Reporting System payment adjustment under the Medicare Shared Savings Program for 2016 and subsequent years, the Medicare Part B Physician Fee Schedule amount for covered professional services furnished during the program year is equal to the applicable percent of the Medicare Part B Physician Fee Schedule amount that would otherwise apply to such services under section 1848 of the Act, as described in § 414.90(e) of this chapter.
(5) The reporting period for a year is the calendar year from January 1 through December 31 that occurs 2 years prior to the program year in which the payment adjustment is applied.
(d) Physician Quality Reporting System payment adjustment for 2017 and 2018.
(1) ACOs, on behalf of eligible professionals who bill under the TIN of an ACO participant, must submit all of the ACO GPRO measures determined under § 425.500 using a CMS web interface, to satisfactorily report on behalf of their eligible professionals for purposes of the Physician Quality Reporting System payment adjustment under the Shared Savings Program for 2017 and 2018.
(2) Eligible professionals who bill under the TIN of an ACO participant within an ACO participate under their ACO participant TIN as a group practice under the Physician Quality Reporting System Group Practice Reporting Option of the Shared Savings Program for purposes of the Physician Quality Reporting System payment adjustment under the Shared Savings Program for 2017 and 2018.
(3) If an ACO, on behalf of eligible professionals who bill under the TIN of an ACO participant, does not satisfactorily report for purposes of the Physician Quality Reporting System payment adjustment for 2017 or 2018, each eligible professional who bills under the TIN of an ACO participant will receive a payment adjustment, as described in § 414.90(e) of this chapter, unless such eligible professionals have reported quality measures apart from the ACO in the form and manner required by the Physician Quality Reporting System.
(4) For eligible professionals subject to the Physician Quality Reporting System payment adjustment under the Medicare Shared Savings Program for 2017 or 2018, the Medicare Part B Physician Fee Schedule amount for covered professional services furnished during the program year is equal to the applicable percent of the Medicare Part B Physician Fee Schedule amount that would otherwise apply to such services under section 1848 of the Act, as described in § 414.90(e) of this chapter.
(5) The reporting period for a year is the calendar year from January 1 through December 31 that occurs 2 years prior to the program year in which the payment adjustment is applied, unless otherwise specified by CMS under the Physician Quality Reporting System.
[76 FR 67973, Nov. 2, 2011, as amended at 77 FR 69372, Nov. 16, 2012; 78 FR 74283, Dec. 10, 2013; 80 FR 71386, Nov. 16, 2015; 81 FR 80560, Nov. 15, 2016]
§ 425.506 Incorporating reporting requirements related to adoption of certified electronic health record technology.
(a) ACOs, ACO participants, and ACO providers/suppliers are encouraged to develop a robust EHR infrastructure.
(b) For performance years 2012 through 2018, as part of the quality performance score, the quality measure regarding EHR adoption will be measured based on a sliding scale.
(c) For performance years 2012 through 2018, performance on this measure will be weighted twice that of any other measure for scoring purposes and for determining compliance with quality performance requirements for domains.
(d) Through reporting period 2016, eligible professionals participating in an ACO under the Shared Savings Program satisfy the CQM reporting component of meaningful use for the Medicare EHR Incentive Program when the following occurs:
(1) The eligible professional extracts data necessary for the ACO to satisfy the quality reporting requirements under this subpart from certified EHR technology.
(2) The ACO reports the ACO GPRO measures through a CMS web interface.
(e) For 2017 and 2018, CMS will annually assess the degree of use of certified EHR technology by eligible clinicians billing through the TINs of ACO participants for purposes of meeting the CEHRT criterion necessary for Advanced Alternative Payment Models under the Quality Payment Program.
(1) During years in which the measure is designated as pay for reporting, in order to demonstrate complete and accurate reporting, at least one eligible clinician billing through the TIN of an ACO participant must meet the reporting requirements under the Advancing Clinical Information category under the Quality Payment Program.
(2) During years in which the measure is designated as pay for performance, the quality measure regarding EHR adoption will be measured based on a sliding scale.
(f) For performance years starting on January 1, 2019, and subsequent performance years, ACOs in a track that—
(1) Does not meet the financial risk standard to be an Advanced APM must certify annually that the percentage of eligible clinicians participating in the ACO that use CEHRT to document and communicate clinical care to their patients or other health care providers meets or exceeds 50 percent; or
(2) Meets the financial risk standard to be an Advanced APM must certify annually that the percentage of eligible clinicians participating in the ACO that use CEHRT to document and communicate clinical care to their patients or other health care providers meets or exceeds the threshold established under § 414.1415(a)(1)(i) of this chapter.
[76 FR 67973, Nov. 2, 2011, as amended at 79 FR 68009, Nov. 13, 2014; 81 FR 80560, Nov. 15, 2016; 83 FR 60094, Nov. 23, 2018]
§ 425.508 Incorporating quality reporting requirements related to the Quality Payment Program.
(a) For performance years (or a performance period) beginning in 2017-2020. ACOs, on behalf of eligible clinicians who bill under the TIN of an ACO participant, must submit all of the CMS web interface measures determined under § 425.500 to satisfactorily report on behalf of their eligible clinicians for purposes of the quality performance category of the Quality Payment Program.
(b) For performance years beginning on or after January 1, 2021. ACOs must submit the quality data via the Alternative Payment Model Performance Pathway (APP) established under § 414.1367 of this chapter, to satisfactorily report on behalf of the eligible clinicians who bill under the TIN of an ACO participant for purposes of the MIPS Quality performance category of the Quality Payment Program.
[81 FR 80561, Nov. 15, 2016, as amended at 85 FR 85040, Dec. 28, 2020]
§ 425.510 Application of the Alternative Payment Model Performance Pathway (APP) to Shared Savings Program ACOs for performance years beginning on or after January 1, 2021.
(a) General.
(1) CMS establishes quality performance measures to assess the quality of care furnished by the ACO. If the ACO demonstrates to CMS that it has satisfied the quality performance requirements in this subpart, and the ACO meets all other applicable requirements, the ACO is eligible to receive shared savings.
(2) CMS seeks to improve the quality of care furnished by ACOs over time by specifying higher standards, new measures, or both.
(b) Quality reporting. ACOs must report quality data via the APP established under § 414.1367 of this chapter, according to the method of submission established by CMS.
(c) Audit and validation of data. CMS retains the right to audit and validate quality data reported by an ACO under paragraph (b) of this section according to § 414.1390 of this chapter.
[85 FR 85041, Dec. 28, 2020]
§ 425.512 Determining the ACO quality performance standard for performance years beginning on or after January 1, 2021.
(a) Establishing a quality performance standard -
(1) Overall standard. The quality performance standard is the overall standard the ACO must meet in order to be eligible to receive shared savings for a performance year. An ACO will not qualify to share in savings in any year it fails to meet the quality performance standard.
(2) For performance year 2022 and subsequent performance years. For the first performance year of an ACO's first agreement period under the Shared Savings Program, if the ACO meets the data completeness requirement at § 414.1340 of this chapter and case minimum requirement at § 414.1380 of this chapter on the three measures it is actively required to report and fields a CAHPS for MIPS survey via the APP, the ACO will meet the quality performance standard.
(3) For performance years 2021 and 2022 -
(i) Designation of quality performance standard. For all ACOs, except as specified in paragraph (a)(2) of this section, CMS designates the quality performance standard as the ACO reporting quality data via the APP established under § 414.1367 of this chapter, according to the method of submission established by CMS and achieving a quality performance score that is equivalent to or higher than the 30th percentile across all MIPS Quality performance category scores, excluding entities/providers eligible for facility-based scoring.
(ii) For performance year 2021. If an ACO does not report any of the ten CMS Web Interface measures or any of the three measures it is actively required to report and does not field a CAHPS for MIPS survey via the APP, the ACO will not meet the quality performance standard.
(iii) For performance year 2022. If an ACO does not report any of the three measures it is actively required to report and does not field a CAHPS for MIPS survey via the APP, the ACO will not meet the quality performance standard.
(4) For performance years 2023 and subsequent performance years.
(i) For all ACOs, except as specified in paragraph (a)(2) of this section, CMS designates the quality performance standard as the ACO reporting quality data via the APP established under § 414.1367 of this chapter, according to the method of submission established by CMS and achieving a quality performance score that is equivalent to or higher than the 40th percentile across all MIPS Quality performance category scores, excluding entities/providers eligible for facility-based scoring.
(ii) If an ACO does not report any of the three measures it is actively required to report and does not field a CAHPS for MIPS survey via the APP, the ACO will not meet the quality performance standard.
(b) Extreme and uncontrollable circumstances. For performance year 2021 and subsequent performance years, including the applicable quality data reporting period for the performance year, CMS uses an alternative approach to calculating the quality score for ACOs affected by extreme and uncontrollable circumstances instead of the methodology specified in paragraph (a) of this section as follows:
(1) CMS determines the ACO was affected by an extreme and uncontrollable circumstance based on either of the following:
(i) Twenty percent or more of the ACO's assigned beneficiaries reside in an area identified under the Quality Payment Program as being affected by an extreme and uncontrollable circumstance.
(A) Assignment is determined under subpart E of this part.
(B) In making this determination, CMS uses the quarter four list of assigned beneficiaries.
(ii) The ACO's legal entity is located in an area identified under the Quality Payment Program as being affected by an extreme and uncontrollable circumstance. An ACO's legal entity location is based on the address on file for the ACO in CMS' ACO application and management system.
(2) If CMS determines the ACO meets the requirements of paragraph (b)(1) of this section, CMS calculates the ACO's quality score as follows:
(i) For performance years 2021 and 2022, the ACO's minimum quality performance score is set to the equivalent of the 30th percentile MIPS Quality performance category score for the relevant performance year as determined under paragraph (a)(3) of this section.
(ii) For performance year 2023 and subsequent performance years, the ACO's minimum quality performance score is set to the equivalent of the 40th percentile MIPS Quality performance category score for the relevant performance year as determined under paragraph (a)(4) of this section.
(3) If the ACO reports quality data via the APP and meets data completeness and case minimum requirements:
(i) For performance years 2021 and 2022, CMS will use the higher of the ACO's quality performance score or the equivalent of the 30th percentile MIPS Quality performance category score for the relevant performance year.
(ii) For performance year 2023 and subsequent performance years, CMS will use the higher of the ACO's quality performance score or the equivalent of the 40th percentile MIPS Quality performance category score for the relevant performance year.
(4) CMS applies determinations made under the Quality Payment Program with respect to -
(i) Whether an extreme and uncontrollable circumstance has occurred; and
(ii) The affected areas.
(5) CMS has sole discretion to determine the time period during which an extreme and uncontrollable circumstance occurred, the percentage of the ACO's assigned beneficiaries residing in the affected areas, and the location of the ACO legal entity.
[85 FR 85041, Dec. 28, 2020]
Subpart G - Shared Savings and Losses
§ 425.600 Selection of risk model.
(a) An ACO may elect to operate under one of the following tracks:
(1) Track 1. For agreement periods beginning before July 1, 2019, an ACO in Track 1 operates under the one-sided model (as described under § 425.604) for the agreement period.
(2) Track 2. For agreement periods beginning before July 1, 2019, an ACO in Track 2 operates under a two-sided model (as described under § 425.606), sharing both savings and losses with the Medicare program for the agreement period.
(3) ENHANCED track. An ACO in the ENHANCED track operates under a two-sided model (as described under § 425.610), sharing both savings and losses with the Medicare program for the agreement period. For purposes of this part, all references to the ENHANCED track are deemed to include Track 3.
(4) BASIC track. For agreement periods beginning on July 1, 2019, and in subsequent years, an ACO in the BASIC track operates under either a one-sided model or a two-sided model (as described under § 425.605), either sharing savings only or sharing both savings and losses with the Medicare program, as specified in this paragraph (a)(4).
(i) Levels of the BASIC track's glide path -
(A) Phase-in of levels of the risk and reward. Under the BASIC track's glide path, the level of risk and potential reward phases in over the course of the agreement period in the following order:
(1) Level A. The ACO operates under a one-sided model as described under § 425.605(d)(1)(i).
(2) Level B. The ACO operates under a one-sided model as described under § 425.605(d)(1)(ii).
(3) Level C. The ACO operates under a two-sided model as described under § 425.605(d)(1)(iii).
(4) Level D. The ACO operates under a two-sided model as described under § 425.605(d)(1)(iv).
(5) Level E. The ACO operates under a two-sided model as described under § 425.605(d)(1)(v).
(B) Glide path progression.
(1) Experience in Track 1.
(i) Except for an ACO that previously participated in Track 1 under paragraph (a)(1) of this section or a new ACO identified as a re-entering ACO because more than 50 percent of its ACO participants have recent prior experience in a Track 1 ACO, an ACO eligible to enter the BASIC track's glide path as determined under paragraphs (d)(1)(i) and (d)(2)(i) of this section may elect to enter its agreement period at any of the levels of risk and potential reward available under paragraphs (a)(4)(i)(A)(1) through (5) of this section.
(ii) An ACO that previously participated in Track 1 under paragraph (a)(1) of this section or a new ACO identified as a re-entering ACO because more than 50 percent of its ACO participants have recent prior experience in a Track 1 ACO may elect to enter its agreement period at any of the levels of risk and potential reward available under paragraphs (a)(4)(i)(A)(2) through (5) of this section.
(2) Automatic advancement. Unless the ACO elects to transition to a higher level of risk and potential reward within the BASIC track's glide path as provided in § 425.226(a)(2)(i), the ACO is automatically advanced to the next level of the BASIC track's glide path at the start of each subsequent performance year of the agreement period, if a higher level of risk and potential reward is available under the BASIC track.
(i) Exception for ACO entering the BASIC track's glide path for an agreement period beginning on July 1, 2019. The automatic advancement does not apply at the start of the second performance year for an ACO entering the BASIC track's glide path for an agreement period beginning on July 1, 2019. For performance year 2020, the ACO remains in the same level of the BASIC track's glide path that it entered for the July 1, 2019 through December 31, 2019 performance year, unless the ACO chooses to advance more quickly in accordance with § 425.226(a)(2)(i). The ACO is automatically advanced to the next level of the BASIC track's glide path at the start of performance year 2021 and all subsequent performance years of the agreement period.
(ii) Exception for new legal entity identified as a low revenue ACO. An exception is available for a low revenue ACO that is a new legal entity and is not identified as a re-entering ACO that enters the BASIC track's glide path at Level A under paragraph (a)(4)(i)(A)(1) of this section, and is automatically advanced to Level B under paragraph (a)(4)(i)(A)(2) of this section for performance year 2 (or performance 3 in the case of ACOs entering an agreement period beginning on July 1, 2019). Prior to the automatic advancement of the ACO to Level C under paragraph (a)(4)(i)(A)(3) of this section, the ACO may elect to remain in Level B under paragraph (a)(4)(i)(A)(2) of this section for performance year 3 (performance year 4 in the case of ACOs entering an agreement period beginning on July 1, 2019). In the case of an ACO that elects to remain in Level B for an additional performance year pursuant to the second sentence of paragraph (a)(4)(i)(B)(2)(ii) of this section, the ACO is automatically advanced to Level E under paragraph (a)(4)(i)(A)(5) of this section at the start of performance year 4 (or performance year 5 in the case of ACOs entering an agreement period beginning on July 1, 2019).
(iii) Exception for ACOs participating in the BASIC track's glide path that elect to maintain their participation level for performance year 2021. Prior to the automatic advancement for performance year 2021, an ACO that is participating in the BASIC track's glide path for performance year 2020 may elect to remain in the same level of the BASIC track's glide path that it entered for the 2020 performance year, for performance year 2021. For performance year 2022, the ACO is automatically advanced to the level of the BASIC track's glide path to which the ACO would have automatically advanced absent the election to maintain its participation level for performance year 2021, unless the ACO elects to transition to a higher level of risk and potential reward within the BASIC track's glide path as provided in § 425.226(a)(2)(i). A voluntary election by an ACO under this paragraph must be made in the form and manner and by a deadline established by CMS.
(iv) Prior to entering performance-based risk, an ACO must meet all requirements to participate under performance-based risk, including establishing an adequate repayment mechanism as specified under § 425.204(f) and selecting a MSR/MLR from the options specified under § 425.605(b).
(3) If the ACO fails to meet the requirements to participate under performance-based risk under paragraph (a)(4)(i)(B)(2)(iii) of this section, the agreement is terminated.
(4) If, in accordance with § 425.226(a)(2)(i), the ACO elects to transition to a higher level of risk and reward available under paragraphs (a)(4)(i)(A)(3) through (5) of this section, then the automatic transition to levels of higher risk and reward specified in paragraph (a)(4)(i)(B)(2) of this section applies to all subsequent performance years of the agreement period.
(ii) Agreement period under Level E of the BASIC track. If an ACO enters the BASIC track and is ineligible to participate under the glide path described in paragraph (a)(4)(i) of this section, as determined under paragraph (d) of this section, Level E as described in paragraph (a)(4)(i)(A)(5) of this section applies to all performance years of the agreement period.
(b) For agreement periods beginning before July 1, 2019, ACOs may operate under the one-sided model for a maximum of 2 agreement periods. An ACO may not operate under the one-sided model for a second agreement period unless the -
(1) Immediately preceding agreement period was under the one-sided model; and
(2) The ACO meets the criteria established for ACOs seeking to renew their agreements under § 425.224(b).
(c) For agreement periods beginning before July 1, 2019, an ACO experiencing a net loss during a previous agreement period may reapply to participate under the conditions in § 425.202(a), except the ACO must also identify in its application the cause(s) for the net loss and specify what safeguards are in place to enable the ACO to potentially achieve savings in its next agreement period.
(d) For agreement periods beginning on July 1, 2019, and in subsequent years, CMS determines an ACO's eligibility for the Shared Savings Program participation options specified in paragraph (a) of this section as follows:
(1) If an ACO is identified as a high revenue ACO, the ACO is eligible for the participation options indicated in paragraph (a) of this section as follows:
(i) If the ACO is determined to be inexperienced with performance-based risk Medicare ACO initiatives, the ACO may enter either the BASIC track's glide path at any of the levels of risk and potential reward available under paragraphs (a)(4)(i)(A)(1) through (5) of this section, except as provided in paragraph (a)(4)(i)(B) of this section, or the ENHANCED track under paragraph (a)(3) of this section.
(ii) If the ACO is determined to be experienced with performance-based risk Medicare ACO initiatives:
(A) The ACO may enter the ENHANCED track under paragraph (a)(3) of this section except as provided in paragraph (d)(1)(ii)(B) of this section.
(B) An ACO in a first or second agreement period beginning in 2016 or 2017 identified as experienced with performance-based risk Medicare ACO initiatives based on participation in the Track 1+ Model may renew for a consecutive agreement period beginning on July 1, 2019, or January 1, 2020 (respectively), under either the BASIC track Level E under paragraph (a)(4)(i)(A)(5) of this section, or the ENHANCED track under paragraph (a)(3) of this section.
(2) If an ACO is identified as a low revenue ACO, the ACO is eligible for the participation options indicated in paragraph (a) of this section as follows:
(i) If the ACO is determined to be inexperienced with performance-based risk Medicare ACO initiatives, the ACO may enter either the BASIC track's glide path at any of the levels of risk and potential reward available under paragraphs (a)(4)(i)(A)(1) through (5) of this section, except as provided in paragraph (a)(4)(i)(B) of this section, or the ENHANCED track under paragraph (a)(3) of this section.
(ii) If the ACO is determined to be experienced with performance-based risk Medicare ACO initiatives, the ACO may enter under either the BASIC track Level E under paragraph (a)(4)(i)(A)(5) of this section, except as provided in paragraph (d)(3) of this section, or the ENHANCED track under paragraph (a)(3) of this section.
(3) Low revenue ACOs may participate under the BASIC track for a maximum of two agreement periods. A low revenue ACO may only participate in the BASIC track for a second agreement period if it satisfies either of the following:
(i) The ACO is the same legal entity as a current or previous ACO that previously entered into a participation agreement for participation in the BASIC track only one time.
(ii) For a new ACO identified as a re-entering ACO, the ACO in which the majority of the new ACO's participants were participating previously entered into a participation agreement for participation in the BASIC track only one time.
(e) CMS monitors low revenue ACOs identified as experienced with performance-based risk Medicare ACO initiatives, during an agreement period in the BASIC track, for changes in the revenue of ACO participants that would cause the ACO to be considered a high revenue ACO and ineligible for participation in the BASIC track. If the ACO meets the definition of a high revenue ACO (as specified in § 425.20) -
(1) The ACO is permitted to complete the remainder of its current performance year under the BASIC track, but is ineligible to continue participation in the BASIC track after the end of that performance year if it continues to meet the definition of a high revenue ACO; and
(2) CMS takes compliance action as specified in §§ 425.216 and 425.218, up to and including termination of the participation agreement, to ensure the ACO does not continue in the BASIC track for subsequent performance years of the agreement period if it continues to meet the definition of a high revenue ACO.
(f) For agreement periods beginning on July 1, 2019, and in subsequent years, CMS determines the agreement period an ACO is entering for purposes of applying program requirements that phase-in over multiple agreement periods, as follows:
(1) An ACO entering an initial agreement period is considered to be entering a first agreement period in the Shared Savings Program.
(2) A re-entering ACO is considered to be entering a new agreement period in the Shared Savings Program as follows -
(i) An ACO whose participation agreement expired without having been renewed re-enters the program under the next consecutive agreement period in the Shared Savings Program;
(ii) An ACO whose participation agreement was terminated under § 425.218 or § 425.220 re-enters the program at the start of the same agreement period in which it was participating at the time of termination from the Shared Savings Program, beginning with the first performance year of that agreement period; or
(iii) A new ACO identified as a re-entering ACO enters the program in an agreement period that is determined based on the prior participation of the ACO in which the majority of the new ACO's participants were participating.
(A) If the participation agreement of the ACO used in this determination expired without having been renewed or was terminated, the agreement period of the re-entering ACO is determined in accordance with paragraph (f)(2)(i) or (ii) of this section, as applicable.
(B) If the ACO used in this determination is currently participating in the program, the new ACO is considered to be entering into the same agreement period as this currently participating ACO, beginning with the first performance year of that agreement period.
(3) A renewing ACO is considered to be entering the next consecutive agreement period in the Shared Savings Program.
(4) For purposes of this paragraph (f), program requirements that phase in over multiple agreement periods are as follows:
(i) The quality performance standard as described in § 425.502(a) or § 425.512(a), as applicable.
(ii) The weight used in calculating the regional adjustment to the ACO's historical benchmark as described in § 425.601(f).
(iii) The use of equal weights to weight each benchmark year as specified in § 425.601(e).
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32841, June 9, 2015; 83 FR 68069, Dec. 31, 2018; 85 FR 27625, May 8, 2020; 85 FR 85041, Dec. 28, 2020]
§ 425.601 Establishing, adjusting, and updating the benchmark for agreement periods beginning on July 1, 2019, and in subsequent years.
(a) Computing per capita Medicare Part A and Part B benchmark expenditures for an ACO's first agreement period. For agreement periods beginning on July 1, 2019, and in subsequent years, in computing an ACO's historical benchmark for its first agreement period under the Shared Savings Program, CMS determines the per capita Parts A and B fee-for-service expenditures for beneficiaries that would have been assigned to the ACO in any of the 3 most recent years prior to the start of the agreement period using the ACO participant TINs identified before the start of the agreement period as required under § 425.118(a) and the beneficiary assignment methodology selected by the ACO for the first performance year of the agreement period as required under § 425.226(a)(1). CMS does all of the following:
(1) Calculates the payment amounts included in Parts A and B fee-for-service claims using a 3-month claims run out with a completion factor.
(i) This calculation excludes indirect medical education (IME) and disproportionate share hospital (DSH) payments.
(ii) This calculation includes individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(2) Makes separate expenditure calculations for each of the following populations of beneficiaries: ESRD, disabled, aged/dual eligible Medicare and Medicaid beneficiaries and aged/non-dual eligible Medicare and Medicaid beneficiaries.
(3) Adjusts expenditures for changes in severity and case mix using prospective HCC risk scores.
(4) Truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures for assignable beneficiaries identified for the 12-month calendar year corresponding to each benchmark year in order to minimize variation from catastrophically large claims.
(5) Trends forward expenditures for each benchmark year (BY1 and BY2) to the third benchmark year (BY3) dollars using a blend of national and regional growth rates.
(i) To trend forward the benchmark, CMS makes separate calculations for expenditure categories for each of the following populations of beneficiaries:
(A) ESRD.
(B) Disabled.
(C) Aged/dual eligible Medicare and Medicaid beneficiaries.
(D) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(ii) National growth rates are computed using CMS Office of the Actuary national Medicare expenditure data for each of the years making up the historical benchmark for assignable beneficiaries identified for the 12-month calendar year corresponding to each benchmark year.
(iii) Regional growth rates are computed using expenditures for the ACO's regional service area for each of the years making up the historical benchmark as follows:
(A) Determine the counties included in the ACO's regional service area based on the ACO's assigned beneficiary population for the relevant benchmark year.
(B) Determine the ACO's regional expenditures as specified under paragraphs (c) and (d) of this section.
(iv) The national and regional growth rates are blended together by taking a weighted average of the two. The weight applied to the -
(A) National growth rate is calculated as the share of assignable beneficiaries in the ACO's regional service area for BY3 that are assigned to the ACO in BY3, as calculated in paragraph (a)(5)(v) of this section; and
(B) Regional growth rate is equal to 1 minus the weight applied to the national growth rate.
(v) CMS calculates the share of assignable beneficiaries in the ACO's regional service area that are assigned to the ACO by doing all of the following:
(A) Calculating the county-level share of assignable beneficiaries that are assigned to the ACO for each county in the ACO's regional service area.
(B) Weighting the county-level shares according to the ACO's proportion of assigned beneficiaries in the county, determined by the number of the ACO's assigned beneficiaries residing in the county in relation to the ACO's total number of assigned beneficiaries.
(C) Aggregating the weighted county-level shares for all counties in the ACO's regional service area.
(6) Restates BY1 and BY2 trended and risk adjusted expenditures using BY3 proportions of ESRD, disabled, aged/dual eligible Medicare and Medicaid beneficiaries and aged/non-dual eligible Medicare and Medicaid beneficiaries.
(7) Weights each year of the benchmark for an ACO's initial agreement period using the following percentages:
(i) BY3 at 60 percent.
(ii) BY2 at 30 percent.
(iii) BY1 at 10 percent.
(8) Adjusts the historical benchmark based on the ACO's regional service area expenditures, making separate calculations for the following populations of beneficiaries: ESRD, disabled, aged/dual eligible Medicare and Medicaid beneficiaries, and aged/non-dual eligible Medicare and Medicaid beneficiaries. CMS does all of the following:
(i) Calculates an average per capita amount of expenditures for the ACO's regional service area as follows:
(A) Determines the counties included in the ACO's regional service area based on the ACO's BY3 assigned beneficiary population.
(B) Determines the ACO's regional expenditures as specified under paragraphs (c) and (d) of this section for BY3.
(C) Adjusts for differences in severity and case mix between the ACO's assigned beneficiary population and the assignable beneficiary population for the ACO's regional service area identified for the 12-month calendar year that corresponds to BY3.
(ii) Calculates the adjustment as follows:
(A) Determines the difference between the average per capita amount of expenditures for the ACO's regional service area as specified under paragraph (a)(8)(i) of this section and the average per capita amount of the ACO's historical benchmark determined under paragraphs (a)(1) through (7) of this section, for each of the following populations of beneficiaries:
(1) ESRD.
(2) Disabled.
(3) Aged/dual eligible for Medicare and Medicaid.
(4) Aged/non-dual eligible for Medicare and Medicaid.
(B) Applies a percentage, as determined in paragraph (f) of this section.
(C) Caps the per capita dollar amount for each Medicare enrollment type (ESRD, Disabled, Aged/dual eligible Medicare and Medicaid beneficiaries, Aged/non-dual eligible Medicare and Medicaid beneficiaries) calculated under paragraph (a)(8)(ii)(B) of this section at a dollar amount equal to 5 percent of national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program in BY3 for assignable beneficiaries in that enrollment type identified for the 12-month calendar year corresponding to BY3 using data from the CMS Office of the Actuary.
(1) For positive adjustments, the per capita dollar amount for a Medicare enrollment type is capped at 5 percent of the national per capita expenditure amount for the enrollment type for BY3.
(2) For negative adjustments, the per capita dollar amount for a Medicare enrollment type is capped at negative 5 percent of the national per capita expenditure amount for the enrollment type for BY3.
(9) For the second and each subsequent performance year during the term of the agreement period, the ACO's benchmark is adjusted for the following, as applicable: For the addition and removal of ACO participants or ACO providers/suppliers in accordance with § 425.118(b), for a change to the ACO's beneficiary assignment methodology selection under § 425.226(a)(1), and for a change to the beneficiary assignment methodology specified in subpart E of this part. To adjust the benchmark, CMS does the following:
(i) Takes into account the expenditures of beneficiaries who would have been assigned to the ACO in any of the 3 most recent years prior to the start of the agreement period.
(ii) Redetermines the regional adjustment amount under paragraph (a)(8) of this section, according to the ACO's assigned beneficiaries for BY3.
(10) The historical benchmark is further adjusted at the time of reconciliation for a performance year to account for changes in severity and case mix of the ACO's assigned beneficiary population as described under §§ 425.605(a), 425.609(c), and 425.610(a).
(b) Updating the benchmark. For all agreement periods beginning on July 1, 2019, and in subsequent years, CMS updates the historical benchmark annually for each year of the agreement period using a blend of national and regional growth rates.
(1) To update the benchmark, CMS makes separate calculations for expenditure categories for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(2) National growth rates are computed using CMS Office of the Actuary national Medicare expenditure data for BY3 and the performance year for assignable beneficiaries identified for the 12-month calendar year corresponding to each year.
(3) Regional growth rates are computed using expenditures for the ACO's regional service area for BY3 and the performance year, computed as follows:
(i) Determine the counties included in the ACO's regional service area based on the ACO's assigned beneficiary population for the year.
(ii) Determine the ACO's regional expenditures as specified under paragraphs (c) and (d) of this section.
(4) The national and regional growth rates are blended together by taking a weighted average of the two. The weight applied to the -
(i) National growth rate is calculated as the share of assignable beneficiaries in the ACO's regional service area that are assigned to the ACO for the applicable performance year as specified in paragraph (a)(5)(v) of this section; and
(ii) Regional growth rate is equal to 1 minus the weight applied to the national growth rate.
(c) Calculating county expenditures. For all agreement periods beginning on July 1, 2019, and in subsequent years, CMS does all of the following to determine risk adjusted county fee-for-service expenditures for use in calculating the ACO's regional fee-for-service expenditures:
(1)
(i) Determines average county fee-for-service expenditures based on expenditures for the assignable population of beneficiaries in each county in the ACO's regional service area, where assignable beneficiaries are identified for the 12-month calendar year corresponding to the relevant benchmark or performance year.
(ii) Makes separate expenditure calculations for each of the following populations of beneficiaries:
(A) ESRD.
(B) Disabled.
(C) Aged/dual eligible Medicare and Medicaid beneficiaries.
(D) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(2) Calculates assignable beneficiary expenditures using the payment amounts included in Parts A and B fee-for-service claims with dates of service in the 12-month calendar year for the relevant benchmark or performance year, using a 3-month claims run out with a completion factor. The calculation -
(i) Excludes IME and DSH payments; and
(ii) Considers individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(3) Truncates a beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures for assignable beneficiaries identified for the 12-month calendar year that corresponds to the relevant benchmark or performance year, in order to minimize variation from catastrophically large claims.
(4) Adjusts fee-for-service expenditures for severity and case mix of assignable beneficiaries in the county using prospective HCC risk scores. The calculation is made according to the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(d) Calculating regional expenditures. For all agreement periods beginning on July 1, 2019, and in subsequent years, CMS calculates an ACO's risk adjusted regional expenditures by -
(1) Weighting the risk-adjusted county-level fee-for-service expenditures determined under paragraph (c) of this section according to the ACO's proportion of assigned beneficiaries in the county, determined by the number of the ACO's assigned beneficiaries in the applicable population (according to Medicare enrollment type) residing in the county in relation to the ACO's total number of assigned beneficiaries in the applicable population (according to Medicare enrollment type) for the relevant benchmark or performance year for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries;
(2) Aggregating the values determined under paragraph (d)(1) of this section for each population of beneficiaries (according to Medicare enrollment type) across all counties within the ACO's regional service area; and
(3) Weighting the aggregate expenditure values determined for each population of beneficiaries (according to Medicare enrollment type) under paragraph (d)(2) of this section by a weight reflecting the proportion of the ACO's overall beneficiary population in the applicable Medicare enrollment type for the relevant benchmark or performance year.
(e) Resetting the benchmark.
(1) An ACO's benchmark is reset at the start of each subsequent agreement period.
(2) For second or subsequent agreements periods beginning on July 1, 2019, and in subsequent years, CMS establishes, adjusts, and updates the rebased historical benchmark in accordance with paragraphs (a) through (d) of this section with the following modifications:
(i) Rather than weighting each year of the benchmark using the percentages provided in paragraph (a)(7) of this section, each benchmark year is weighted equally.
(ii) For a renewing ACO or re-entering ACO whose prior agreement period benchmark was calculated according to § 425.603(c), to determine the weight used in the regional adjustment calculation described in paragraph (f) of this section, CMS considers the agreement period the ACO is entering into according to § 425.600(f) in combination with either of the following -
(A) The weight previously applied to calculate the regional adjustment to the ACO's benchmark under § 425.603(c)(9) in its most recent prior agreement period; or
(B) For a new ACO identified as a re-entering ACO, CMS considers the weight previously applied to calculate the regional adjustment to the benchmark under § 425.603(c)(9) in its most recent prior agreement period of the ACO in which the majority of the new ACO's participants were participating previously.
(f) Phase-in of weights used in regional adjustment calculation.
(1) The first time that an ACO's benchmark is adjusted based on the ACO's regional service area expenditures, CMS calculates the regional adjustment as follows:
(i) Using 35 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's initial or rebased historical benchmark, if the ACO is determined to have lower spending than the ACO's regional service area.
(ii) Using 15 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's initial or rebased historical benchmark, if the ACO is determined to have higher spending than the ACO's regional service area.
(2) The second time that an ACO's benchmark is adjusted based on the ACO's regional service area expenditures, CMS calculates the regional adjustment as follows:
(i) Using 50 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark if the ACO is determined to have lower spending than the ACO's regional service area.
(ii) Using 25 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark if the ACO is determined to have higher spending than the ACO's regional service area.
(3) The third time that an ACO's benchmark is adjusted based on the ACO's regional service area expenditures, CMS calculates the regional adjustment as follows:
(i) Using 50 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark if the ACO is determined to have lower spending than the ACO's regional service area.
(ii) Using 35 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark if the ACO is determined to have higher spending than the ACO's regional service area.
(4) The fourth or subsequent time that an ACO's benchmark is adjusted based on the ACO's regional service area expenditures, CMS calculates the regional adjustment to the historical benchmark using 50 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark.
(5) To determine if an ACO has lower or higher spending compared to the ACO's regional service area, CMS does the following:
(i) Multiplies the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's historical benchmark for each population of beneficiaries (ESRD, Disabled, Aged/dual eligible Medicare and Medicaid beneficiaries, Aged/non-dual eligible Medicare and Medicaid beneficiaries) as calculated under either paragraph (a)(8)(ii)(A) or (e) of this section by the applicable proportion of the ACO's assigned beneficiary population (ESRD, Disabled, Aged/dual eligible Medicare and Medicaid beneficiaries, Aged/non-dual eligible Medicare and Medicaid beneficiaries) for BY3 of the historical benchmark.
(ii) Sums the amounts determined in paragraph (f)(4)(i) of this section across the populations of beneficiaries (ESRD, Disabled, Aged/dual eligible Medicare and Medicaid beneficiaries, Aged/non-dual eligible Medicare and Medicaid beneficiaries).
(iii) If the resulting sum is a net positive value, the ACO is considered to have lower spending compared to the ACO's regional service area. If the resulting sum is a net negative value, the ACO is considered to have higher spending compared to the ACO's regional service area.
(iv) If during the term of the agreement period CMS adjusts the ACO's benchmark, as specified in paragraph (a)(9) of this section, CMS redetermines whether the ACO is considered to have lower spending or higher spending compared to the ACO's regional service area for purposes of determining the percentage in paragraphs (f)(1) and (2) of this section used in calculating the adjustment under either paragraph (a)(8) or (e) of this section.
(g) July 1, 2019 through December 31, 2019 performance year. In determining performance for the July 1, 2019 through December 31, 2019 performance year described in § 425.609(c), CMS does all of the following:
(1) When adjusting the benchmark using the methodology set forth in paragraph (a)(10) of this section and § 425.609(c), CMS adjusts for severity and case mix between BY3 and CY 2019.
(2) When updating the benchmark using the methodology set forth in paragraph (b) of this section and § 425.609(c), CMS updates the benchmark based on growth between BY3 and CY 2019.
[83 FR 68071, Dec. 31, 2018, as amended at 85 FR 85042, Dec. 28, 2020]
§ 425.602 Establishing, adjusting, and updating the benchmark for an ACO's first agreement period beginning on or before January 1, 2018.
(a) Computing per capita Medicare Part A and Part B benchmark expenditures. For agreement periods beginning on or before January 1, 2018, in computing an ACO's fixed historical benchmark that is adjusted for historical growth and beneficiary characteristics, including health status, CMS determines the per capita Parts A and B fee-for-service expenditures for beneficiaries that would have been assigned to the ACO in any of the 3 most recent years prior to the agreement period using the ACO participants' TINs identified at the start of the agreement period. CMS does all of the following:
(1) Calculates the payment amounts included in Parts A and B fee-for-service claims using a 3-month claims run out with a completion factor.
(i) This calculation excludes indirect medical education (IME) and disproportionate share hospital (DSH) payments.
(ii) This calculation considers individually beneficiary identifiable payments made under a demonstration, pilot or time limited program.
(A) For agreement periods beginning before 2018, this calculation considers all individually beneficiary identifiable payments, including interim payments, made under a demonstration, pilot or time limited program.
(B) For agreement periods beginning in 2018, this calculation considers individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(C) For the 2018 performance year and subsequent performance years in agreement periods beginning in 2015, 2016 and 2017, the benchmark is adjusted to reflect only individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(2) Makes separate expenditure calculations for each of the following populations of beneficiaries: ESRD, disabled, aged/dual eligible Medicare and Medicaid beneficiaries and aged/non-dual eligible Medicare and Medicaid beneficiaries.
(3) Adjusts expenditures for changes in severity and case mix using prospective HCC risk scores.
(4) Truncation of expenditures:
(i) For agreement periods beginning before 2017—
(A) Truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures as determined for each benchmark year in order to minimize variation from catastrophically large claims; and
(B) For the 2017 performance year and any subsequent performance years in agreement periods beginning in 2014, 2015 and 2016, the benchmark is adjusted to reflect the use of assignable beneficiaries in determining the 99th percentile of Medicare fee-for-service expenditures for purposes of truncating expenditures for assigned beneficiaries during each benchmark year as specified in paragraph (a)(4)(ii) of this section.
(ii) For agreement periods beginning in 2017 and 2018, truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures for assignable beneficiaries identified for the 12-month calendar year corresponding to each benchmark year in order to minimize variation from catastrophically large claims.
(5) Trending expenditures:
(i) For agreement periods beginning before 2017—
(A) Using CMS Office of the Actuary national Medicare expenditure data for each of the years making up the historical benchmark, determines national growth rates and trends expenditures for each benchmark year (BY1 and BY2) to the third benchmark year (BY3) dollars.
(B) To trend forward the benchmark, CMS makes separate calculations for expenditure categories for each of the following populations of beneficiaries:
(1) ESRD.
(2) Disabled.
(3) Aged/dual eligible Medicare and Medicaid beneficiaries.
(4) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(C) For the 2017 performance year and any subsequent performance years in agreement periods beginning in 2014, 2015 and 2016, the benchmark is adjusted to reflect the use of assignable beneficiaries to perform each of these calculations as specified in paragraph (a)(5)(ii) of this section.
(ii) For agreement periods beginning in 2017 and 2018—
(A) Using CMS Office of the Actuary national Medicare expenditure data for each of the years making up the historical benchmark, determines national growth rates for assignable beneficiaries identified for the 12-month calendar year corresponding to each benchmark year, and trends expenditures for each benchmark year (BY1 and BY2) to the third benchmark year (BY3) dollars.
(B) To trend forward the benchmark, CMS makes separate calculations for expenditure categories for each of the following populations of beneficiaries:
(1) ESRD.
(2) Disabled.
(3) Aged/dual eligible Medicare and Medicaid beneficiaries.
(4) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(6) Restates BY1 and BY2 trended and risk adjusted expenditures in BY3 proportions of ESRD, disabled, aged/dual eligible Medicare and Medicaid beneficiaries and aged/non-dual eligible Medicare and Medicaid beneficiaries.
(7) Weights each year of the benchmark for the initial agreement period using the following percentages:
(i) BY3 at 60 percent.
(ii) BY2 at 30 percent.
(iii) BY1 at 10 percent.
(8) The ACO's benchmark is adjusted for the addition and removal of ACO participants or ACO providers/suppliers in accordance with § 425.118(b) and for a change to the beneficiary assignment methodology specified in subpart E of this part, as applicable, to take into account the expenditures for beneficiaries who would have been assigned to the ACO in any of the 3 most recent years prior to the start of the agreement period.
(9) The historical benchmark is further adjusted at the time of reconciliation for a performance year to account for changes in severity and case mix for newly and continuously assigned beneficiaries using prospective HCC risk scores and demographic factors as described under §§ 425.604(a)(1) through (3), 425.606(a)(1) through (3), and 425.610(a)(1) through (3).
(b) Updating the benchmark. CMS updates the historical benchmark annually for each year of the agreement period based on the flat dollar equivalent of the projected absolute amount of growth in national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program.
(1) For performance years before 2017, CMS updates the historical benchmark annually for each year of the agreement period based on the flat dollar equivalent of the projected absolute amount of growth in national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program.
(i) CMS updates the fixed benchmark by the projected absolute amount of growth in national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program using data from CMS' Office of the Actuary.
(ii) To update the benchmark, CMS makes expenditure calculations for separate categories for each of the following populations of beneficiaries:
(A) ESRD.
(B) Disabled.
(C) Aged/dual eligible Medicare and Medicaid beneficiaries.
(D) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(2) For the 2017 performance year and subsequent performance years, CMS updates the historical benchmark annually for each year of the agreement period based on the flat dollar equivalent of the projected absolute amount of growth in national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program for assignable beneficiaries identified for the 12-month calendar year corresponding to the year for which the update is calculated.
(i) CMS updates the fixed benchmark by the projected absolute amount of growth in national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program for assignable beneficiaries identified for the 12-month calendar year corresponding to the year for which the update is being calculated using data from CMS' Office of the Actuary.
(ii) To update the benchmark, CMS makes expenditure calculations for separate categories for each of the following populations of beneficiaries:
(A) ESRD.
(B) Disabled.
(C) Aged/dual eligible Medicare and Medicaid beneficiaries.
(D) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(c) January 1, 2019 through June 30, 2019 performance year. In determining performance for the January 1, 2019 through June 30, 2019 performance year described in § 425.609(b) CMS does all of the following:
(1) When adjusting the benchmark using the methodology set forth in paragraph (a)(9) of this section and § 425.609(b), CMS adjusts for severity and case mix between BY3 and CY 2019.
(2) When updating the benchmark using the methodology set forth in paragraph (b) of this section and § 425.609(b), CMS updates the benchmark based on growth between BY3 and CY 2019.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32842, June 9, 2015; 81 FR 38014, June 10, 2016; 82 FR 53370, Nov. 15, 2017; 83 FR 60094, Nov. 23, 2018; 83 FR 68074, Dec. 31, 2018; 85 FR 85042, Dec. 28, 2020]
§ 425.603 Resetting, adjusting, and updating the benchmark for a subsequent agreement period beginning on or before January 1, 2019.
(a) An ACO's benchmark is reset at the start of each subsequent agreement period.
(b) For second agreement periods beginning in 2016, CMS establishes, adjusts, and updates the rebased historical benchmark in accordance with § 425.602(a) and (b) with the following modifications:
(1) Rather than weighting each year of the benchmark using the percentages provided at § 425.602(a)(7), each benchmark year is weighted equally.
(2) An additional adjustment is made to account for the average per capita amount of savings generated during the ACO's previous agreement period. The adjustment is limited to the average number of assigned beneficiaries (expressed as person years) under the ACO's first agreement period.
(c) For second or subsequent agreement periods beginning in 2017, 2018 and on January 1, 2019, CMS establishes the rebased historical benchmark by determining the per capita Parts A and B fee-for-service expenditures for beneficiaries who would have been assigned to the ACO in any of the 3 most recent years before the agreement period using the certified ACO participant list submitted before the start of the agreement period as required under § 425.118. CMS does all of the following:
(1) Calculates the payment amounts included in Parts A and B fee-for-service claims using a 3-month claims run out with a completion factor. The calculation—
(i) Excludes IME and DSH payments; and
(ii) Considers individually beneficiary identifiable payments made under a demonstration, pilot or time limited program.
(A) For agreement periods beginning before 2018, considers all individually beneficiary identifiable payments, including interim payments, made under a demonstration, pilot or time limited program.
(B) For agreement periods beginning in 2018 and on January 1, 2019, considers individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(C) For the 2018 and 2019 performance years in agreement periods beginning in 2017, the benchmark is adjusted to reflect only individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(2) Makes separate expenditure calculations for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(3) Adjusts expenditures for changes in severity and case mix using prospective HCC risk scores.
(4) Truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures for assignable beneficiaries identified for the 12-month calendar year corresponding to each benchmark year in order to minimize variation from catastrophically large claims.
(5) Trends forward expenditures for each benchmark year (BY1 and BY2) to the third benchmark year (BY3) dollars using regional growth rates based on expenditures for the ACO's regional service area as determined under paragraphs (e) and (f) of this section, making separate expenditure calculations for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(6) Restates BY1 and BY2 trended and risk-adjusted expenditures in BY3 proportions of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(7) Weights each benchmark year equally.
(8) The ACO's benchmark is adjusted for the following, as applicable: For the addition and removal of ACO participants or ACO providers/suppliers in accordance with § 425.118(b), and for a change to the beneficiary assignment methodology specified in subpart E of this part. To adjust the benchmark, CMS does the following:
(i) Takes into account the expenditures for beneficiaries who would have been assigned to the ACO in any of the 3 most recent years prior to the start of the agreement period.
(ii) Redetermines the regional adjustment amount under paragraph (c)(9) of this section, according to the ACO's assigned beneficiaries for BY3.
(9) Adjusts the historical benchmark based on the ACO's regional service area expenditures, making separate calculations for the following populations of beneficiaries: ESRD, disabled, aged/dual eligible Medicare and Medicaid beneficiaries, and aged/non-dual eligible Medicare and Medicaid beneficiaries. CMS does all of the following:
(i) Calculates an average per capita amount of expenditures for the ACO's regional service area as follows:
(A) Determines the counties included in the ACO's regional service area based on the ACO's BY3 assigned beneficiary population.
(B) Determines the ACO's regional expenditures as specified under paragraphs (e) and (f) of this section for BY3.
(C) Adjusts for differences in severity and case mix between the ACO's assigned beneficiary population and the assignable beneficiary population for the ACO's regional service area identified for the 12-month calendar year that corresponds to BY3.
(ii) Calculates the adjustment as follows:
(A) Determines the difference between the average per capita amount of expenditures for the ACO's regional service area as specified under paragraph (c)(9)(i) of this section and the average per capita amount of the ACO's rebased historical benchmark determined under paragraphs (c)(1) through)(8) of this section, for each of the following populations of beneficiaries:
(1) ESRD.
(2) Disabled.
(3) Aged/dual eligible Medicare and Medicaid beneficiaries.
(4) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(B) Applies a percentage, determined as follows:
(1) The first time an ACO's benchmark is rebased using the methodology described under paragraph (c) of this section, CMS calculates the regional adjustment as follows:
(i) Using 35 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark, if the ACO is determined to have lower spending than the ACO's regional service area;
(ii) Using 25 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark, if the ACO is determined to have higher spending than the ACO's regional service area.
(2) The second time that an ACO's benchmark is rebased using the methodology described under paragraph (c) of this section, CMS calculates the regional adjustment to the historical benchmark as follows:
(i) Using 70 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark, unless the Secretary determines a lower weight should be applied, if the ACO is determined to have lower spending than the ACO's regional service area;
(ii) Using 50 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark, if the ACO is determined to have higher spending than the ACO's regional service area.
(3) The third or subsequent time that an ACO's benchmark is rebased using the methodology described under paragraph (c) of this section, CMS calculates the regional adjustment to the historical benchmark using 70 percent of the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark, unless the Secretary determines a lower weight should be applied.
(4) To determine if an ACO has lower or higher spending compared to the ACO's regional service area, CMS does the following:
(i) Multiplies the difference between the average per capita amount of expenditures for the ACO's regional service area and the average per capita amount of the ACO's rebased historical benchmark for each population of beneficiaries (ESRD, Disabled, Aged/dual eligible Medicare and Medicaid beneficiaries, Aged/non-dual eligible Medicare and Medicaid beneficiaries) as calculated under paragraph (c)(9)(ii)(A) of this section by the applicable proportion of the ACO's assigned beneficiary population (ESRD, Disabled, Aged/dual eligible Medicare and Medicaid beneficiaries, Aged/non-dual eligible Medicare and Medicaid beneficiaries) for benchmark year 3 of the rebased historical benchmark.
(ii) Sums the amounts determined in paragraph (c)(9)(ii)(B)(4)(i) of this section across the populations of beneficiaries (ESRD, Disabled, Aged/dual eligible Medicare and Medicaid beneficiaries, Aged/non-dual eligible Medicare and Medicaid beneficiaries).
(iii) If the resulting sum is a net positive value, the ACO is considered to have lower spending compared to the ACO's regional service area. If the resulting sum is a net negative value, the ACO is considered to have higher spending compared to the ACO's regional service area.
(iv) If CMS adjusts the ACO's benchmark, as specified in paragraph (c)(8) of this section, CMS redetermines whether the ACO is considered to have lower spending or higher spending compared to the ACO's regional service area for purposes of determining the percentage used in calculating the adjustment in paragraphs (c)(9)(ii)(B)(1) and (2) of this section.
(10) The historical benchmark is further adjusted at the time of reconciliation for a performance year to account for changes in severity and case mix for newly and continuously assigned beneficiaries using prospective HCC risk scores and demographic factors as described under §§ 425.604(a)(1) through (3), 425.606(a)(1) through (3), and 425.610(a)(1) through (3).
(d) For second or subsequent agreement periods beginning in 2017, 2018 and on January 1, 2019, CMS updates the rebased historical benchmark under paragraph (c) of this section, annually for each year of the agreement period by the growth in risk adjusted regional per beneficiary FFS spending for the ACO's regional service area by doing all of the following:
(1) Determining the counties included in the ACO's regional service area based on the ACO's assigned beneficiary population used to determine financial reconciliation for the relevant performance year.
(2) Determining growth rates based on expenditures for counties in the ACO's regional service area calculated under paragraphs (e) and (f) of this section, for the performance year compared to BY3 for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(3) Updating the benchmark by making separate calculations for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(e) For second or subsequent agreement periods beginning in 2017, 2018 and on January 1, 2019, CMS does all of the following to determine risk adjusted county fee-for-service expenditures for use in calculating the ACO's regional fee-for-service expenditures:
(1)
(i) Determines average county fee-for-service expenditures based on expenditures for the assignable population of beneficiaries in each county, where assignable beneficiaries are identified for the 12-month calendar year corresponding to the relevant benchmark or performance year.
(ii) Makes separate expenditure calculations for each of the following populations of beneficiaries:
(A) ESRD.
(B) Disabled.
(C) Aged/dual eligible Medicare and Medicaid beneficiaries.
(D) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(2) Calculates assignable beneficiary expenditures using the payment amounts included in Parts A and B fee-for-service claims with dates of service in the 12-month calendar year for the relevant benchmark or performance year, using a 3-month claims run out with a completion factor. The calculation—
(i) Excludes IME and DSH payments; and
(ii) Considers individually beneficiary identifiable payments made under a demonstration, pilot or time limited program.
(A) For agreement periods beginning before 2018, considers all individually beneficiary identifiable payments, including interim payments, made under a demonstration, pilot or time limited program.
(B) For agreement periods beginning in 2018 and on January 1, 2019, considers individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(C) For the 2018 and 2019 performance years in agreement periods beginning in 2017, risk adjusted county fee-for-service expenditures are adjusted to reflect only individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(3) Truncates a beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures for assignable beneficiaries identified for the 12-month calendar year that corresponds to the relevant benchmark or performance year, in order to minimize variation from catastrophically large claims.
(4) Adjusts fee-for-service expenditures for severity and case mix of assignable beneficiaries in the county using prospective CMS-HCC risk scores. The calculation is made according to the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(f) For second or subsequent agreement periods beginning in 2017, 2018, and on January 1, 2019, CMS calculates an ACO's risk adjusted regional expenditures by—
(1) Weighting the risk-adjusted county-level fee-for-service expenditures determined under paragraph (e) of this section according to the ACO's proportion of assigned beneficiaries in the county, determined by the number of the ACO's assigned beneficiaries in the applicable population (according to Medicare enrollment type) residing in the county in relation to the ACO's total number of assigned beneficiaries in the applicable population (according to Medicare enrollment type) for the relevant benchmark or performance year for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(2) Aggregating the values determined under paragraph (f)(1) of this section for each population of beneficiaries (according to Medicare enrollment type) across all counties within the ACO's regional service area; and
(3) Weighting the aggregate expenditure values determined for each population of beneficiaries (according to Medicare enrollment type) under paragraph (f)(2) of this section by a weight reflecting the proportion of the ACO's overall beneficiary population in the applicable Medicare enrollment type for the relevant benchmark or performance year.
(g) In determining performance for the January 1, 2019 through June 30, 2019 performance year described in § 425.609(b) CMS does all of the following:
(1) When adjusting the benchmark using the methodology set forth in paragraph (c)(10) of this section and § 425.609(b), CMS adjusts for severity and case mix between BY3 and CY 2019.
(2) When updating the benchmark using the methodology set forth in paragraph (d) of this section and § 425.609(b), CMS updates the benchmark based on growth between BY3 and CY 2019.
[81 FR 38014, June 10, 2016, as amended at 82 FR 53370, Nov. 15, 2017; 83 FR 60094, Nov. 23, 2018; 83 FR 68074, Dec. 31, 2018; 85 FR 85042, Dec. 28, 2020]
§ 425.604 Calculation of savings under the one-sided model.
(a) Savings determination. For each performance year, CMS determines whether the estimated average per capita Medicare expenditures under the ACO for Medicare fee-for-service beneficiaries for Parts A and B services are below the applicable updated benchmark determined under § 425.602 or § 425.603.
(1) Newly assigned beneficiaries. CMS uses an ACO's HCC prospective risk score to adjust the benchmark for changes in severity and case mix in this population.
(2) Continuously assigned beneficiaries.
(i) CMS uses demographic factors to adjust the benchmark for changes in the continuously assigned population.
(ii) If the prospective HCC risk score is lower in the performance year for this population, CMS will adjust the benchmark for changes in severity and case mix in this population using this lower prospective HCC risk score.
(3) Assigned beneficiary changes in demographics and health status are used to adjust benchmark expenditures as described in § 425.602(a) or § 425.603(c). In adjusting the benchmark for health status and demographic changes CMS makes adjustments for separate categories for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(4)
(i) For performance years before 2017 to minimize variation from catastrophically large claims, CMS truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures as determined for each performance year.
(ii) For the 2017 performance year and subsequent performance years, to minimize variation from catastrophically large claims, CMS truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures as determined for the applicable performance year for assignable beneficiaries identified for the 12-month calendar year corresponding to the performance year.
(5) CMS uses a 3 month claims run out with a completion factor to calculate an ACO's per capita expenditures for each performance year.
(6) Calculations of the ACO's expenditures will include the payment amounts included in Part A and B fee-for-service claims.
(i) These calculations will exclude indirect medical education (IME) and disproportionate share hospital (DSH) payments.
(ii) These calculations will take into consideration individually beneficiary identifiable payments made under a demonstration, pilot or time limited program.
(A) For performance years beginning before 2018, these calculations will take into consideration all individually beneficiary identifiable payments, including interim payments, made under a demonstration, pilot or time limited program.
(B) For performance year 2018 and subsequent performance years, these calculations will take into consideration individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(7) In order to qualify for a shared savings payment, the ACO's average per capita Medicare expenditures for the performance year must be below the applicable updated benchmark by at least the minimum savings rate established for the ACO under paragraph (b) of this section.
(b) Minimum savings rate (MSR). CMS uses a sliding scale, based on the number of beneficiaries assigned to the ACO under subpart E of this part, to establish the MSR for an ACO participating under the one-sided model. The MSR under the one-sided model for an ACO based on the number of assigned beneficiaries is as follows:
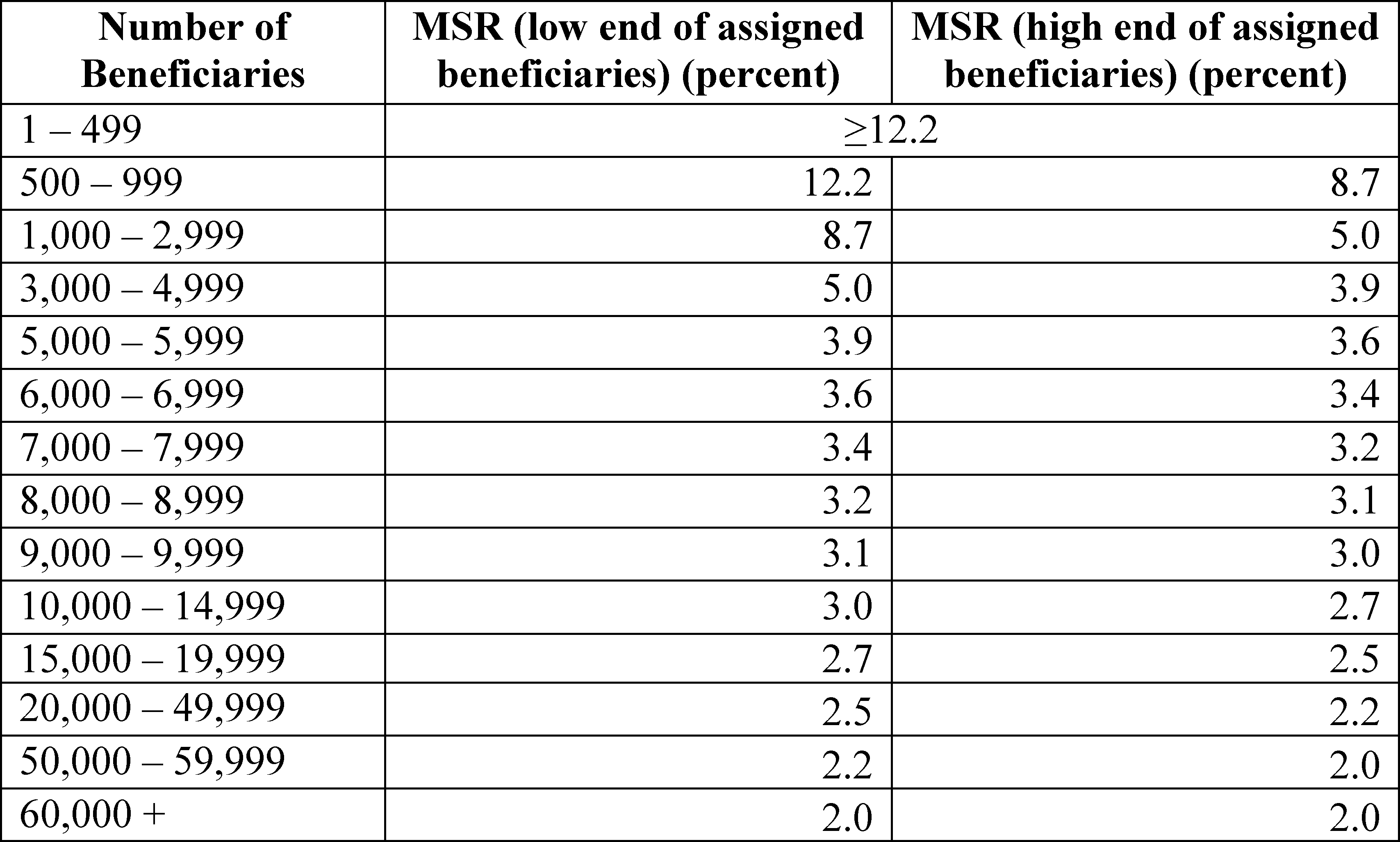
(c) Qualification for shared savings payment —
(1) For performance years (or a performance period) beginning on or before January 1, 2020. In order to qualify for shared savings, an ACO must meet or exceed its minimum savings rate determined under paragraph (b) of this section, meet the minimum quality performance standards established under § 425.502, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(2) For the performance year beginning on January 1, 2021. To qualify for shared savings, an ACO must meet or exceed its minimum savings rate determined under paragraph (b) of this section, meet the quality performance standard established under § 425.512, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(d) Final sharing rate —
(1) For performance years (or a performance period) beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under the one-sided model will receive a shared savings payment of up to 50 percent of all savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (e)(2) of this section).
(2) For the performance year beginning on January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under Track 1 will receive a shared savings payment of 50 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (e)(2) of this section).
(e) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate will apply to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under the one-sided model may not exceed 10 percent of its updated benchmark.
(f) Notification of savings. CMS notifies an ACO in writing regarding whether the ACO qualifies for a shared savings payment, and if so, the amount of the payment due.
(g) January 1, 2019 through June 30, 2019 performance year. Shared savings for the January 1, 2019 through June 30, 2019 performance year are calculated as described in § 425.609.
[76 FR 67973, Nov. 2, 2011, as amended at 81 FR 38016, June 10, 2016; 82 FR 53370, Nov. 15, 2017; 83 FR 60094, Nov. 23, 2018; 83 FR 68074, Dec. 31, 2018; 85 FR 85042, Dec. 28, 2020]
§ 425.605 Calculation of shared savings and losses under the BASIC track.
(a) General rules. For each performance year, CMS determines whether the estimated average per capita Medicare Parts A and B fee-for-service expenditures for Medicare fee-for-service beneficiaries assigned to the ACO are above or below the updated benchmark determined under § 425.601. In order to qualify for a shared savings payment under the BASIC track, or to be responsible for sharing losses with CMS, an ACO's average per capita Medicare Parts A and B fee-for-service expenditures for its assigned beneficiary population for the performance year must be below or above the updated benchmark, respectively, by at least the minimum savings or loss rate under paragraph (b) of this section.
(1) CMS uses an ACO's prospective HCC risk score to adjust the benchmark for changes in severity and case mix in the assigned beneficiary population between BY3 and the performance year.
(i) Positive adjustments in prospective HCC risk scores are subject to a cap of 3 percent.
(ii) This cap is the maximum increase in risk scores for each agreement period, such that any positive adjustment between BY3 and any performance year in the agreement period cannot be larger than 3 percent.
(2) In risk adjusting the benchmark as described in § 425.601(a)(10), CMS makes separate adjustments for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(3) To minimize variation from catastrophically large claims, CMS truncates an assigned beneficiary's total annual Medicare Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare Parts A and B fee-for-service expenditures as determined for the applicable performance year for assignable beneficiaries identified for the 12-month calendar year corresponding to the performance year.
(4) CMS uses a 3-month claims run out with a completion factor to calculate an ACO's per capita expenditures for each performance year.
(5) Calculations of the ACO's expenditures include the payment amounts included in Medicare Parts A and B fee-for-service claims.
(i) These calculations exclude indirect medical education (IME) and disproportionate share hospital (DSH) payments.
(ii) These calculations take into consideration individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(6) In order to qualify for a shared savings payment, the ACO's average per capita Medicare Parts A and B fee-for-service expenditures for the performance year must be below the applicable updated benchmark by at least the minimum savings rate established for the ACO under paragraph (b) of this section.
(b) Minimum savings or loss rate.
(1) For ACOs under a one-sided model of the BASIC track's glide path, as specified under paragraphs (d)(1)(i) and (ii) of this section, CMS uses a sliding scale, based on the number of beneficiaries assigned to the ACO under subpart E of this part, to establish the MSR for the ACO as follows:
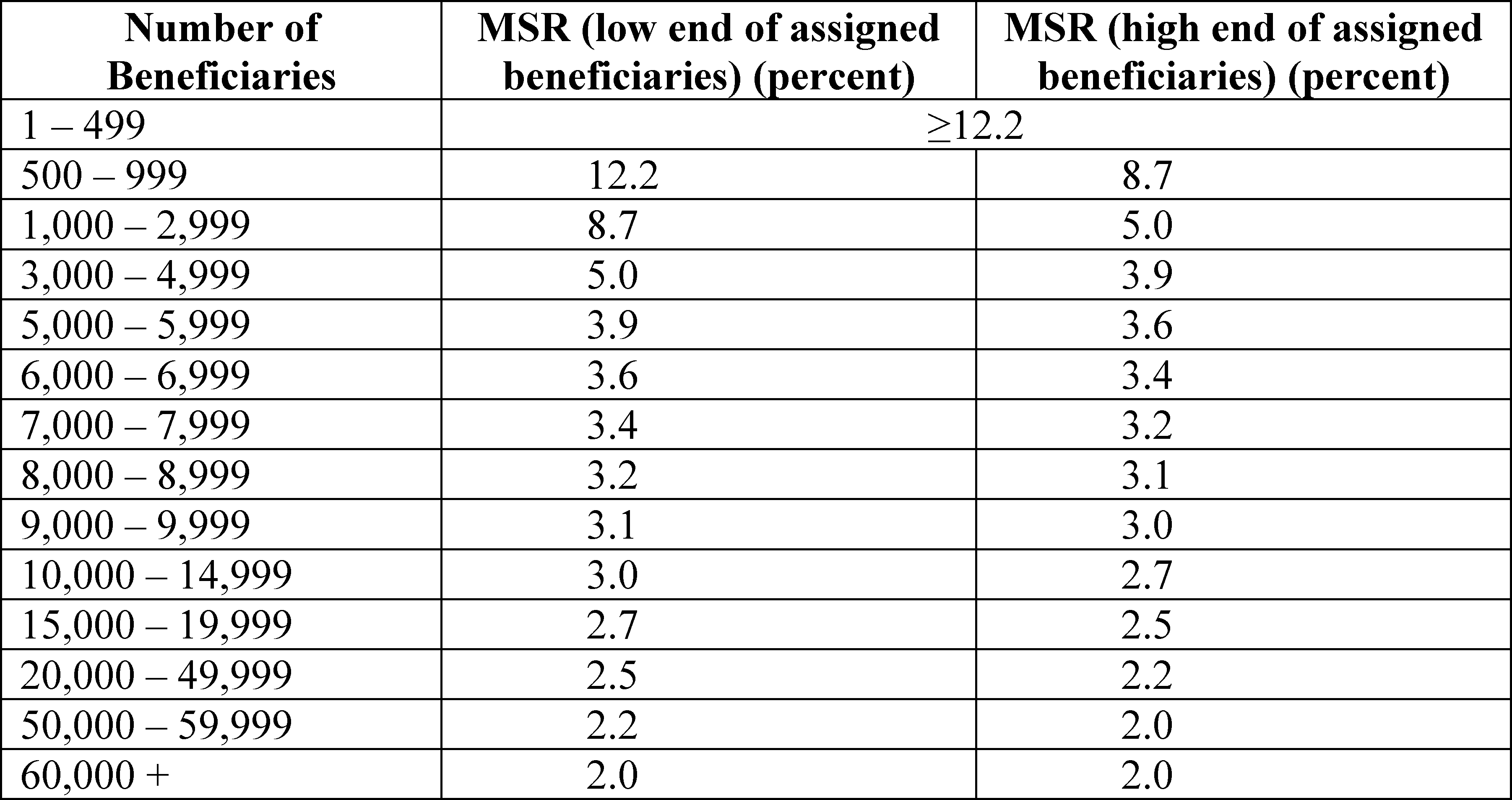
(2) Prior to entering a two-sided model of the BASIC track, the ACO must select the MSR/MLR. For an ACO making this selection as part of an application for, or renewal of, participation in a two-sided model of the BASIC track, the selection applies for the duration of the agreement period under the BASIC track. For an ACO making this selection during an agreement period, as part of the application cycle prior to entering a two-sided model of the BASIC track, the selection applies for the remaining duration of the applicable agreement period under the BASIC track.
(i) The ACO must choose from the following options for establishing the MSR/MLR:
(A) Zero percent MSR/MLR.
(B) Symmetrical MSR/MLR in a 0.5 percent increment between 0.5 and 2.0 percent.
(C) Symmetrical MSR/MLR that varies, based on the number of beneficiaries assigned to the ACO under subpart E of this part. The MSR is the same as the MSR that would apply under paragraph (b)(1) of this section for an ACO under a one-sided model of the BASIC track's glide path, and is based on the number of assigned beneficiaries. The MLR under the BASIC track is equal to the negative MSR.
(ii) The ACO selects its MSR/MLR as part of one the following:
(A) Application for, or renewal of, program participation in a two-sided model of the BASIC track.
(B) Election to participate in a two-sided model of the BASIC track during an agreement period under § 425.226.
(C) Automatic transition from Level B to Level C of the BASIC track's glide path under § 425.600(a)(4)(i).
(D) Automatic transition from Level B to Level E of the BASIC track's glide path under § 425.600(a)(4)(i)(B)(2)(ii).
(3) To qualify for shared savings under the BASIC track, an ACO's average per capita Medicare Parts A and B fee-for-service expenditures for its assigned beneficiary population for the performance year must be below its updated benchmark costs for the year by at least the MSR established for the ACO.
(4) To be responsible for sharing losses with the Medicare program, an ACO's average per capita Medicare Parts A and B fee-for-service expenditures for its assigned beneficiary population for the performance year must be above its updated benchmark costs for the year by at least the MLR established for the ACO.
(c) Qualification for shared savings payment -
(1) For performance years beginning on or before January 1, 2020. To qualify for shared savings, an ACO must meet the minimum savings rate requirement established under paragraph (b) of this section, meet the minimum quality performance standards established under § 425.502, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(2) For performance years beginning on or after January 1, 2021. To qualify for shared savings, an ACO must meet the minimum savings rate requirement established under paragraph (b) of this section, meet the quality performance standard established under § 425.512, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(d) Levels of risk and potential reward.
(1) The following levels of risk and potential reward apply to an ACO in the BASIC track, as permitted under § 425.600(d).
(i) Level A (one-sided model) -
(A) Final sharing rate -
(1) For performance years beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level A, receives a shared savings payment of up to 40 percent of all the savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (d)(1)(i)(B) of this section).
(2) For performance years beginning on or after January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level A, receives a shared savings payment of 40 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (d)(1)(i)(B) of this section).
(B) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate specified in paragraph (d)(1)(i)(A) of this section applies to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under the BASIC track, Level A, may not exceed 10 percent of its updated benchmark.
(ii) Level B (one-sided model) -
(A) Final sharing rate -
(1) For performance years beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level B, receives a shared savings payment of up to 40 percent of all the savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (d)(1)(ii)(B) of this section).
(2) For performance years beginning on or after January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level B, receives a shared savings payment of 40 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (d)(1)(ii)(B) of this section).
(B) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate specified in paragraph (d)(1)(ii)(A) of this section applies to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under the BASIC track, Level B, may not exceed 10 percent of its updated benchmark.
(iii) Level C (two-sided model) -
(A) Final sharing rate -
(1) For performance years beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level C, receives a shared savings payment of up to 50 percent of all the savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (d)(1)(iii)(B) of this section).
(2) For performance years beginning on or after January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level C, receives a shared savings payment of 50 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (d)(1)(iii)(B) of this section).
(B) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate specified in paragraph (d)(1)(iii)(A) of this section applies to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under the BASIC track, Level C may not exceed 10 percent of its updated benchmark.
(C) Shared loss rate. For an ACO that is required to share losses with the Medicare program for expenditures over the updated benchmark, the amount of shared losses is determined based on a fixed 30 percent loss sharing rate.
(D) Loss recoupment limit.
(1) Except as provided in paragraph (d)(1)(iii)(D)(2) of this section, the amount of shared losses for which an eligible ACO is liable may not exceed 2 percent of total Medicare Parts A and B fee-for-service revenue of the ACO participants in the ACO.
(2) Instead of the revenue-based loss recoupment limit determined under paragraph (d)(1)(iii)(D)(1) of this section, the loss recoupment limit for the ACO is 1 percent of the ACO's updated benchmark as determined under § 425.601, if the amount determined under paragraph (d)(1)(iii)(D)(1) of this section exceeds the amount that is 1 percent of the ACO's updated benchmark as determined under § 425.601.
(iv) Level D (two-sided model) -
(A) Final sharing rate -
(1) For performance years beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level D, receives a shared savings payment of up to 50 percent of all the savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (d)(1)(iv)(B) of this section).
(2) For performance years beginning on or after January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level D, receives a shared savings payment of 50 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (d)(1)(iv)(B) of this section).
(B) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate specified in paragraph (d)(1)(iv)(A) of this section applies to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under the BASIC track, Level D, may not exceed 10 percent of its updated benchmark.
(C) Shared loss rate. For an ACO that is required to share losses with the Medicare program for expenditures over the updated benchmark, the amount of shared losses is determined based on a fixed 30 percent loss sharing rate.
(D) Loss recoupment limit.
(1) Except as provided in paragraph (d)(1)(iv)(D)(2) of this section, the amount of shared losses for which an eligible ACO is liable may not exceed 4 percent of total Medicare Parts A and B fee-for-service revenue of the ACO participants in the ACO.
(2) Instead of the revenue-based loss recoupment limit determined under paragraph (d)(1)(iv)(D)(1) of this section, the loss recoupment limit for the ACO is 2 percent of the ACO's updated benchmark as determined under § 425.601, if the amount determined under paragraph (d)(1)(iv)(D)(1) of this section exceeds the amount that is 2 percent of the ACO's updated benchmark as determined under § 425.601.
(v) Level E (two-sided model) -
(A) Final sharing rate -
(1) For performance years beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level E, receives a shared savings payment of up to 50 percent of all the savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (d)(1)(v)(B) of this section).
(2) For performance years beginning on or after January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under the BASIC track, Level E, receives a shared savings payment of 50 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (d)(1)(v)(B) of this section).
(B) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate specified in paragraph (d)(1)(v)(A) of this section applies to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under the BASIC track, Level E, may not exceed 10 percent of its updated benchmark.
(C) Shared loss rate. For an ACO that is required to share losses with the Medicare program for expenditures over the updated benchmark, the amount of shared losses is determined based on a fixed 30 percent loss sharing rate.
(D) Loss recoupment limit.
(1) Except as provided in paragraph (d)(1)(v)(D)(2) of this section, the amount of shared losses for which an eligible ACO is liable may not exceed the percentage, as specified in § 414.1415(c)(3)(i)(A) of this chapter, of total Medicare Parts A and B fee-for-service revenue of the ACO participants in the ACO.
(2) Instead of the revenue-based loss recoupment limit determined under paragraph (d)(1)(v)(D)(1) of this section, the loss recoupment limit for the ACO is 1 percentage point higher than the percentage, as specified in § 414.1415(c)(3)(i)(B) of this chapter, based on the ACO's updated benchmark as determined under § 425.601, if the amount determined under paragraph (d)(1)(v)(D)(1) of this section exceeds this percentage of the ACO's updated benchmark as determined under § 425.601.
(2) Level E risk and reward as specified in paragraph (d)(1)(v) of this section applies to an ACO eligible to enter the BASIC track that is determined to be experienced with performance-based risk Medicare ACO initiatives as specified under § 425.600(d).
(e) Notification of savings and losses.
(1) CMS notifies an ACO in writing regarding whether the ACO qualifies for a shared savings payment, and if so, the amount of the payment due.
(2) CMS provides written notification to an ACO of the amount of shared losses, if any, that it must repay to the program.
(3) If an ACO has shared losses, the ACO must make payment in full to CMS within 90 days of receipt of notification.
(f) Extreme and uncontrollable circumstances. The following adjustment is made in calculating the amount of shared losses, after the application of the shared loss rate and the loss recoupment limit.
(1) CMS determines the percentage of the ACO's performance year assigned beneficiary population affected by an extreme and uncontrollable circumstance.
(2) CMS reduces the amount of the ACO's shared losses by an amount determined by multiplying the shared losses by the percentage of the total months in the performance year affected by an extreme and uncontrollable circumstance, and the percentage of the ACO's assigned beneficiaries who reside in an area affected by an extreme and uncontrollable circumstance.
(i) For an ACO that is liable for a pro-rated share of losses under § 425.221(b)(2)(ii), the amount of shared losses determined for the performance year during which the termination becomes effective is adjusted according to this paragraph (f)(2).
(ii) [Reserved]
(3) CMS applies determinations made under the Quality Payment Program with respect to -
(i) Whether an extreme and uncontrollable circumstance has occurred; and
(ii) The affected areas.
(4) CMS has sole discretion to determine the time period during which an extreme and uncontrollable circumstance occurred and the percentage of the ACO's assigned beneficiaries residing in the affected areas.
(g) July 1, 2019 through December 31, 2019 performance year. Shared savings or shared losses for the July 1, 2019 through December 31, 2019 performance year are calculated as described in § 425.609.
[83 FR 68075, Dec. 31, 2018, as amended at 85 FR 85042, Dec. 28, 2020]
§ 425.606 Calculation of shared savings and losses under Track 2.
(a) General rule. For each performance year, CMS determines whether the estimated average per capita Medicare expenditures under the ACO for Medicare fee-for-service beneficiaries for Parts A and B services are above or below the updated benchmark determined under § 425.602 or § 425.603. In order to qualify for a shared savings payment under Track 2, or to be responsible for sharing losses with CMS, an ACO's average per capita Medicare expenditures under the ACO for Medicare fee-for-service beneficiaries for Parts A and B services for the performance year must be below or above the updated benchmark, respectively, by at least the minimum savings or loss rate under paragraph (b) of this section.
(1) Newly assigned beneficiaries. CMS uses an ACO's HCC prospective risk score to adjust the benchmark for changes in severity and case mix in this population.
(2) Continuously assigned beneficiaries.
(i) CMS uses demographic factors to adjust the benchmark for changes in the continuously assigned beneficiary population.
(ii) If the prospective HCC risk score is lower in the performance year for this population, CMS will adjust the benchmark for changes in severity and case mix for this population using this lower prospective HCC risk score.
(3) Assigned beneficiary changes in demographics and health status are used to adjust benchmark expenditures as described in § 425.602(a) or § 425.603(c). In adjusting the benchmark for health status and demographic changes CMS makes separate adjustments for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(4)
(i) For performance years before 2017 to minimize variation from catastrophically large claims, CMS truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures as determined for each performance year.
(ii) For the 2017 performance year and subsequent performance years, to minimize variation from catastrophically large claims, CMS truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures as determined for the applicable performance year for assignable beneficiaries identified for the 12-month calendar year corresponding to the performance year.
(5) CMS uses a 3 month claims run out with a completion factor to calculate an ACO's per capita expenditures for each performance year.
(6) Calculations of the ACO's expenditures will include the payment amounts included in Part A and B fee-for-service claims.
(i) These calculations will exclude indirect medical education (IME) and disproportionate share hospital (DSH) payments.
(ii) These calculations will take into consideration individually beneficiary identifiable payments made under a demonstration, pilot or time limited program.
(A) For performance years beginning before 2018, these calculations will take into consideration all individually beneficiary identifiable payments, including interim payments, made under a demonstration, pilot or time limited program.
(B) For performance year 2018 and subsequent performance years, these calculations will take into consideration individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(7) In order to qualify for a shared savings payment, the ACO's average per capita Medicare expenditures for the performance year must be below the applicable updated benchmark by at least the minimum savings rate established for the ACO under paragraph (b) of this section.
(b) Minimum savings or loss rate.
(1)
(i) For agreement periods beginning in 2012 through 2015, the ACO's MSR and MLR are set at 2 percent.
(ii) For agreement periods beginning in 2016 and subsequent years, as part of the ACO's application for, or renewal of, program participation, the ACO must choose from the following options for establishing the MSR/MLR for the duration of the agreement period:
(A) Zero percent MSR/MLR.
(B) Symmetrical MSR/MLR in a 0.5 percent increment between 0.5-2.0 percent.
(C) Symmetrical MSR/MLR that varies, based on the number of beneficiaries assigned to the ACO under subpart E of this part. The MSR for an ACO under Track 2 is the same as the MSR that would apply in the one-sided model under § 425.604(b) and is based on the number of assigned beneficiaries. The MLR under Track 2 is equal to the negative MSR.
(2) To qualify for shared savings under Track 2, an ACO's average per capita Medicare expenditures for the performance year must be below its updated benchmark costs for the year by at least the MSR established for the ACO.
(3) To be responsible for sharing losses with the Medicare program, an ACO's average per capita Medicare expenditures for the performance year must be above its updated benchmark costs for the year by at least the MLR established for the ACO.
(c) Qualification for shared savings payment —
(1) For performance years (or a performance period) beginning on or before January 1, 2020. To qualify for shared savings, an ACO must meet the minimum savings rate requirement established under paragraph (b) of this section, meet the minimum quality performance standards established under § 425.502, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(2) For the performance year beginning on January 1, 2021. To qualify for shared savings, an ACO must meet the minimum savings rate requirement established under paragraph (b) of this section, meet the quality performance standard established under § 425.512, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(d) Final sharing rate —
(1) For performance years (or a performance period) beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under Track 2 will receive a shared savings payment of up to 60 percent of all the savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (e)(2) of this section).
(2) For the performance year beginning on January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under Track 2 will receive a shared savings payment of 60 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (e)(2) of this section).
(e) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate will apply to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under Track 2 may not exceed 15 percent of its updated benchmark.
(f) Shared loss rate —
(1) For performance years (or a performance period) beginning on or before January 1, 2020. For an ACO that is required to share losses with the Medicare program for expenditures over the updated benchmark, the amount of shared losses is determined based on the inverse of its final sharing rate described in paragraph (d)(1) of this section (that is, 1 minus the final shared savings rate determined under paragraph (d)(1) of this section). The shared loss rate—
(i) May not exceed 60 percent; and
(ii) May not be less than 40 percent.
(2) For the performance year beginning on January 1, 2021. For an ACO that is required to share losses with the Medicare program for expenditures over the updated benchmark, the amount of shared losses is determined as follows:
(i) If the ACO meets the quality performance standard established in § 425.512, CMS determines the shared loss rate as follows:
(A) Calculate the quotient of the MIPS Quality performance category points earned divided by the total MIPS Quality performance category points available.
(B) Calculate the product of the quotient determined in paragraph (f)(2)(i)(A) of this section and 60 percent.
(C) Calculate the shared loss rate as 1 minus the product determined in paragraph (f)(2)(i)(B) of this section. The shared loss rate—
(1) May not exceed 60 percent; and
(2) May not be less than 40 percent.
(ii) If the ACO fails to meet the quality performance standard established in § 425.512, the shared loss rate is 60 percent.
(g) Loss recoupment limit. The amount of shared losses for which an eligible ACO is liable may not exceed the following percentages of its updated benchmark as determined under § 425.602 or § 425.603:
(1) 5 percent in the first performance year of participation in Track 2 under the Shared Savings Program.
(2) 7.5 percent in the second performance year.
(3) 10 percent in the third and any subsequent performance year.
(h) Notification of savings and losses.
(1) CMS notifies an ACO in writing regarding whether the ACO qualifies for a shared savings payment, and if so, the amount of the payment due.
(2) CMS provides written notification to an ACO of the amount of shared losses, if any, that it must repay to the program.
(3) If an ACO has shared losses, the ACO must make payment in full to CMS within 90 days of receipt of notification.
(i) Extreme and uncontrollable circumstances. For performance year 2017 and subsequent performance years, the following adjustment is made in calculating the amount of shared losses, after the application of the shared loss rate in paragraph (f) of this section and the loss recoupment limit in paragraph (g) of this section.
(1) CMS determines the percentage of the ACO's performance year assigned beneficiary population affected by an extreme and uncontrollable circumstance.
(2) CMS reduces the amount of the ACO's shared losses by an amount determined by multiplying the shared losses by the percentage of the total months in the performance year affected by an extreme and uncontrollable circumstance, and the percentage of the ACO's assigned beneficiaries who reside in an area affected by an extreme and uncontrollable circumstance.
(i) For an ACO that is liable for a pro-rated share of losses under § 425.221(b)(2)(ii) or (b)(3)(i), the amount of shared losses determined for the performance year during which the termination becomes effective is adjusted according to this paragraph (i)(2).
(ii) [Reserved]
(3) CMS applies determinations made under the Quality Payment Program with respect to—
(i) Whether an extreme and uncontrollable circumstance has occurred; and
(ii) The affected areas.
(4) CMS has sole discretion to determine the time period during which an extreme and uncontrollable circumstance occurred and the percentage of the ACO's assigned beneficiaries residing in the affected areas.
(j) January 1, 2019 through June 30, 2019. Shared savings or shared losses for the January 1, 2019 through June 30, 2019 performance year are calculated as described in § 425.609.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32842, June 9, 2015; 81 FR 38017, June 10, 2016; 82 FR 53370, Nov. 15, 2017; 82 FR 60918, Dec. 26, 2017; 83 FR 60094, Nov. 23, 2018; 83 FR 68077, Dec. 31, 2018; 85 FR 85043, Dec. 28, 2020]
§ 425.608 Determining first year performance for ACOs beginning April 1 or July 1, 2012.
(a) For April 1 and July 1, 2012 starters, first year (defined as 21 and 18 months respectively) performance will be based on an optional interim payment calculation (based on the ACO's first 12 months of participation) and a final reconciliation at the end of the ACO's first performance year. Unless stated otherwise, for purposes of the interim payment calculation and first year reconciliation, the methodology under subpart E of this part for assigning beneficiaries and the methodology described in § 425.602 through § 425.606 for calculating shared savings and losses will apply, and quality performance will be assessed as described in subpart F of this part.
(b) In the interim payment calculation, based on the ACO's first 12 months of performance—
(1) CMS compares the first 12 months of per capita beneficiary expenditures to a historical benchmark updated for the period which includes the ACO's first 12 months of participation, taking into account changes in health status and demographics; and
(2) Quality performance is based on GPRO quality data reported for CY 2012.
(c)
(1) The interim payment calculation is reconciled with the ACO's performance for its complete first performance year, defined as 21 months for April 1, 2012 starters and 18 months for July 1, 2012 starters.
(2) The first year reconciliation takes into account expenditures spanning the entire 21 or 18 months of the first performance year.
(3) First performance year expenditures are summed over beneficiaries assigned in two overlapping 12 month assignment windows.
(i) The first window will be the first 12 months used for interim payment calculation.
(ii) The second window will be CY2013.
(4) Expenditures for the first performance year are the sum of aggregate expenditure dollars accounting for the ACO's first 6 or 9 months of performance within CY 2012 for beneficiaries assigned for the interim payment calculation and aggregate dollars calculated for CY2013 for beneficiaries assigned for CY 2013.
(5) Adjustments for health status and demographic changes are performed as described in § 425.604 through § 425.606 with the following exceptions:
(i) Beneficiaries from the CY2013 assignment window are identified as continuously assigned or newly assigned relative to the previous calendar year.
(ii) The adjustment factor identified for purposes of the interim payment calculation is applied to the 6 months or 9 months of the ACO's first performance year that lie within CY2012.
(6) The updated benchmark, stated in aggregate dollars, is the sum of the interim updated benchmark for the average fraction of expenditures incurred in the latter 6 or 9 months of CY 2012 and an updated aggregate benchmark representing CY 2013.
(7) A savings percentage (based on a comparison of summed expenditures to summed updated benchmark dollars) for the ACO's 18 or 21 month performance year is compared to the ACO's MSR or MLR. The reconciled amount of the shared savings or losses owed to or by the ACO for the performance year is net of any interim payments of shared savings or losses.
(8) Quality performance for the first year reconciliation is based on complete and accurate reporting, of all required quality measures, for CYs 2012 and 2013.
(d) An ACO with a start date of April 1, 2012 or July 1, 2012 has the option to request an interim payment calculation based on quality and financial performance for its first 12 months of program participation. As required under § 425.204(f), the ACO requesting an interim payment calculation must have a mechanism in place to pay back the interim payment if final reconciliation determines an overpayment.
(e) Unless otherwise stated, program requirements which apply in the course of a performance year apply to the interim payment calculation and first year reconciliation.
§ 425.609 Determining performance for 6-month performance years during CY 2019.
(a) General. An ACO's financial and quality performance for a 6-month performance year during 2019 are determined as described in this section.
(b) January 2019 through June 2019. For ACOs participating in a 6-month performance year from January 1, 2019, through June 30, 2019, under § 425.200(b)(2)(ii)(B) and for ACOs eligible for pro-rated shared savings or liable for pro-rated shared losses in accordance with § 425.221(b)(3)(i) for the performance period from January 1, 2019, through June 30, 2019, CMS reconciles the ACO for the period from January 1, 2019, through June 30, 2019, after the conclusion of CY 2019, based on the 12-month calendar year and pro-rates shared savings or shared losses to reflect the ACO's participation from January 1, 2019, through June 30, 2019. CMS does all of the following to determine financial and quality performance:
(1) Uses the ACO participant list in effect for the performance year beginning January 1, 2019, to determine beneficiary assignment, using claims for the entire calendar year, as specified in §§ 425.402 and 425.404, and according to the ACO's track as specified in § 425.400.
(i) For ACOs under preliminary prospective assignment with retrospective reconciliation the assignment window is CY 2019.
(ii) For ACOs under prospective assignment—
(A) Medicare fee-for-service beneficiaries are prospectively assigned to the ACO based on the beneficiary's use of primary care services in the most recent 12 months for which data are available; and
(B) Beneficiaries remain prospectively assigned to the ACO at the end of CY 2019 if they do not meet any of the exclusion criteria under § 425.401(b) during the calendar year.
(2) Uses the ACO's quality performance for the 2019 reporting period to determine the ACO's quality performance score as specified in § 425.502.
(i) The ACO participant list finalized for the first performance year of the ACO's agreement period beginning on July 1, 2019, is used to determine the quality reporting samples for the 2019 reporting year for the following ACOs:
(A) An ACO that extends its participation agreement for a 6-month performance year from January 1, 2019, through June 30, 2019, under § 425.200(b)(2)(ii)(B), and enters a new agreement period beginning on July 1, 2019.
(B) An ACO that participates in the program for the first 6 months of a 12-month performance year during 2019 and is eligible for pro-rated shared savings or liable for pro-rated shared losses in accordance with § 425.221(b)(3)(i).
(ii) The ACO's latest certified ACO participant list is used to determine the quality reporting samples for the 2019 reporting year for an ACO that extends its participation agreement for the 6-month performance year from January 1, 2019, through June 30, 2019, under § 425.200(b)(2)(ii)(B), and does not enter a new agreement period beginning on July 1, 2019.
(3) Uses the methodology for calculating shared savings or shared losses applicable to the ACO under the terms of the participation agreement that was in effect on January 1, 2019.
(i) The ACO's historical benchmark is determined according to either § 425.602 (first agreement period) or § 425.603 (second agreement period) except as follows:
(A) The benchmark is adjusted for changes in severity and case mix between BY3 and CY 2019 using the methodology that accounts separately for newly and continuously assigned beneficiaries using prospective HCC risk scores and demographic factors as described under §§ 425.604(a)(1) through (3), 425.606(a)(1) through (3), and 425.610(a)(1) through (3).
(B) The benchmark is updated to CY 2019 according to the methodology described under § 425.602(b), § 425.603(b), or § 425.603(d), based on whether the ACO is in its first or second agreement period, and for an ACO in a second agreement period, the date on which that agreement period began.
(ii) The ACO's financial performance is determined based on the track the ACO is participating under during the performance year starting on January 1, 2019 (§ 425.604, § 425.606 or § 425.610), unless otherwise specified. In determining ACO financial performance, CMS does all of the following:
(A) Average per capita Medicare Parts A and B fee-for-service expenditures for CY 2019 are calculated for the ACO's performance year assigned beneficiary population identified in paragraph (b)(1) of this section.
(B) Expenditures calculated in paragraph (b)(3)(ii)(A) of this section are compared to the ACO's updated benchmark determined according to paragraph (b)(3)(i) of this section.
(C)
(1) The ACO's performance year assigned beneficiary population identified in paragraph (b)(1) of this section is used to determine the MSR for Track 1 ACOs and the variable MSR/MLR for ACOs in a two-sided model that selected this option at the start of their agreement period. For two-sided model ACOs that selected a fixed MSR/MLR at the start of the ACO's agreement period, this fixed MSR/MLR is applied. In the event an ACO's performance year assigned population identified in paragraph (b)(1) of this section is below 5,000 beneficiaries, the MSR/MLR is determined according to § 425.110(b).
(2) To qualify for shared savings an ACO must do all of the following:
(i) Have average per capita Medicare Parts A and B fee-for-service expenditures for its assigned beneficiary population for CY 2019 below its updated benchmark costs for the year by at least the MSR established for the ACO based on the track the ACO is participating under during the performance year starting on January 1, 2019 (§ 425.604, § 425.606 or § 425.610) and paragraph (b)(3)(ii)(C)(1) of this section.
(ii) Meet the minimum quality performance standards established under § 425.502 and according to paragraph (b)(2) of this section.
(iii) Otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(3) To be responsible for sharing losses with the Medicare program, an ACO's average per capita Medicare Parts A and B fee-for-service expenditures for its assigned beneficiary population for CY 2019 must be above its updated benchmark costs for the year by at least the MLR established for the ACO based on the track the ACO is participating under during the performance year starting on January 1, 2019 (§ 425.606 or § 425.610) and paragraph (b)(3)(ii)(C)(1) of this section.
(D) For an ACO that meets all the requirements to receive a shared savings payment under paragraph (b)(3)(ii)(C)(2) of this section—
(1) The final sharing rate, determined based on the track the ACO is participating under during the performance year starting on January 1, 2019 (§ 425.604, § 425.606 or § 425.610), is applied to all savings under the updated benchmark specified under paragraph (b)(3)(i) of this section, not to exceed the performance payment limit for the ACO based on its track; and
(2) After applying the applicable performance payment limit, CMS pro-rates any shared savings amount determined under paragraph (b)(3)(ii)(D)(1) of this section by multiplying the amount by one-half, which represents the fraction of the calendar year covered by the period from January 1, 2019, through June 30, 2019.
(E) For an ACO responsible for shared losses under paragraph (b)(3)(ii)(C)(3) of this section—
(1) The shared loss rate, determined based on the track the ACO is participating under during the performance year starting on January 1, 2019 (§ 425.606 or § 425.610), is applied to all losses under the updated benchmark specified under paragraph (b)(3)(i) of this section, not to exceed the loss recoupment limit for the ACO based on its track; and
(2) After applying the applicable loss recoupment limit, CMS pro-rates any shared losses amount determined under paragraph (b)(3)(ii)(E)(1) of this section by multiplying the amount by one-half, which represents the fraction of the calendar year covered by the period from January 1, 2019, through June 30, 2019.
(c) July 2019 through December 2019. For ACOs entering an agreement period beginning on July 1, 2019, the ACO's first performance year is from July 1, 2019, through December 31, 2019, as specified in § 425.200(c)(3). CMS reconciles the ACO for the period from July 1, 2019, through December 31, 2019, after the conclusion of CY 2019, based on the 12-month calendar year and pro-rates shared savings or shared losses to reflect the ACO's participation from July 1, 2019, through December 31, 2019. CMS does all of the following to determine financial and quality performance:
(1) Uses the ACO participant list in effect for the performance year beginning on July 1, 2019, to determine beneficiary assignment, using claims for the entire calendar year, consistent with the methodology the ACO selected at the start of its agreement period under § 425.400(a)(4)(ii).
(i) For ACOs under preliminary prospective assignment with retrospective reconciliation the assignment window is CY 2019.
(ii) For ACOs under prospective assignment—
(A) The assignment window is the same as the assignment window that applies under paragraph (b)(1)(ii)(A) of this section for ACOs under prospective assignment for the 6-month performance year from January 1, 2019, through June 30, 2019; and
(B) Beneficiaries remain prospectively assigned to the ACO at the end of CY 2019 if they do not meet any of the exclusion criteria under § 425.401(b) during the calendar year.
(2) Uses the ACO's quality performance for the 2019 reporting period to determine the ACO's quality performance score as specified in § 425.502. The ACO participant list finalized for the first performance year of the ACO's agreement period beginning on July 1, 2019, is used to determine the quality reporting samples for the 2019 reporting year for all ACOs.
(3) Uses the methodology for calculating shared savings or shared loses applicable to the ACO for its first performance year under its agreement period beginning on July 1, 2019.
(i) The ACO's historical benchmark is determined according to § 425.601 except as follows:
(A) The benchmark is adjusted for changes in severity and case mix between BY3 and CY 2019 based on growth in prospective HCC risk scores, subject to a cap of positive 3 percent as described under § 425.605(a)(1) or § 425.610(a)(2).
(B) The benchmark is updated to CY 2019 according to the methodology described under § 425.601(b).
(ii) The ACO's financial performance is determined based on the track the ACO is participating under during the performance year starting on July 1, 2019 (§ 425.605 (BASIC track) or § 425.610 (ENHANCED track)), unless otherwise specified. In determining ACO financial performance, CMS does all of the following:
(A) Average per capita Medicare Parts A and B fee-for-service expenditures for CY 2019 are calculated for the ACO's performance year assigned beneficiary population identified in paragraph (c)(1) of this section.
(B) Expenditures calculated in paragraph (c)(3)(ii)(A) of this section are compared to the ACO's updated benchmark determined according to paragraph (c)(3)(i) of this section.
(C)
(1) The ACO's performance year assigned beneficiary population identified in paragraph (c)(1) of this section is used to determine the MSR for ACOs in BASIC track Level A or Level B, and the variable MSR/MLR for ACOs in a two-sided model that selected this option at the start of their agreement period. In the event a two-sided model ACO selected a fixed MSR/MLR at the start of its agreement period, and the ACO's performance year assigned population identified in paragraph (c)(1) of this section is below 5,000 beneficiaries, the MSR/MLR is determined based on the number of assigned beneficiaries as specified in § 425.110(b)(3)(iii).
(2) To qualify for shared savings an ACO must do all of the following:
(i) Have average per capita Medicare Parts A and B fee-for-service expenditures for its assigned beneficiary population for CY 2019 below its updated benchmark costs for the year by at least the MSR established for the ACO based on the track the ACO is participating under during the performance year starting on July 1, 2019 (§ 425.605 or § 425.610) and paragraph (c)(3)(ii)(C)(1) of this section.
(ii) Meet the minimum quality performance standards established under § 425.502 and according to paragraph (c)(2) of this section.
(iii) Otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(3) To be responsible for sharing losses with the Medicare program, an ACO's average per capita Medicare Parts A and B fee-for-service expenditures for its assigned beneficiary population for CY 2019 must be above its updated benchmark costs for the year by at least the MLR established for the ACO based on the track the ACO is participating under during the performance year starting on July 1, 2019 (§ 425.605 or § 425.610) and paragraph (c)(3)(ii)(C)(1) of this section.
(D) For an ACO that meets all the requirements to receive a shared savings payment under paragraph (c)(3)(ii)(C)(2) of this section—
(1) The final sharing rate, determined based on the track the ACO is participating under during the performance year starting on July 1, 2019 (§ 425.605 or § 425.610), is applied to all savings under the updated benchmark specified under paragraph (c)(3)(i) of this section, not to exceed the performance payment limit for the ACO based on its track; and
(2) After applying the applicable performance payment limit, CMS pro-rates any shared savings amount determined under paragraph (c)(3)(ii)(D)(1) of this section by multiplying the amount by one-half, which represents the fraction of the calendar year covered by the July 1, 2019 through December 31, 2019 performance year.
(E) For an ACO responsible for shared losses under paragraph (c)(3)(ii)(C)(3) of this section—
(1) The shared loss rate, determined based on the track the ACO is participating under during the performance year starting on July 1, 2019 (§ 425.605 or § 425.610), is applied to all losses under the updated benchmark specified under paragraph (c)(3)(i) of this section, not to exceed the loss recoupment limit for the ACO based on its track; and
(2) After applying the applicable loss recoupment limit, CMS pro-rates any shared losses amount determined under paragraph (c)(3)(ii)(E)(1) of this section by multiplying the amount by one-half, which represents the fraction of the calendar year covered by the July 1, 2019 through December 31, 2019 performance year.
(d) Extreme and uncontrollable circumstances. For ACOs affected by extreme and uncontrollable circumstances during CY 2019—
(1) In calculating the amount of shared losses owed, CMS makes adjustments to the amount determined in paragraph (b)(3)(ii)(E)(1) or (c)(3)(ii)(E)(1) of this section, as specified in § 425.605(f), § 425.606(i), or § 425.610(i), as applicable; and
(2) In determining the ACO's quality performance score for the 2019 quality reporting period, CMS uses the alternative scoring methodology specified in § 425.502(f).
(e) Notification of savings and losses.
(1) CMS notifies the ACO of shared savings or shared losses separately for the January 1, 2019 through June 30, 2019 performance year (or performance period) and the July 1, 2019 through December 31, 2019 performance year, consistent with the notification requirements specified in §§ 425.604(f), 425.605(e), 425.606(h), and 425.610(h), as applicable:
(i) CMS notifies an ACO in writing regarding whether the ACO qualifies for a shared savings payment, and if so, the amount of the payment due.
(ii) CMS provides written notification to an ACO of the amount of shared losses, if any, that it must repay to the program.
(iii) If an ACO has shared losses, the ACO must make payment in full to CMS within 90 days of receipt of notification.
(2) If an ACO is reconciled for both the January 1, 2019 through June 30, 2019 performance year (or performance period) and the July 1, 2019 through December 31, 2019 performance year, CMS issues a separate notice of shared savings or shared losses for each performance year (or performance period), and if the ACO has shared savings for one performance year (or performance period) and shared losses for the other performance year (or performance period), CMS reduces the amount of shared savings by the amount of shared losses.
(i) If any amount of shared savings remains after completely repaying the amount of shared losses owed, the ACO is eligible to receive payment for the remainder of the shared savings.
(ii) If the amount of shared losses owed exceeds the amount of shared savings earned, the ACO is accountable for payment of the remaining balance of shared losses in full.
[83 FR 60094, Nov. 23, 2018, as amended at 83 FR 68078, Dec. 31, 2018]
§ 425.610 Calculation of shared savings and losses under the ENHANCED track.
(a) General rule. For each performance year, CMS determines whether the estimated average per capita Medicare expenditures under the ACO for Medicare fee-for-service beneficiaries for Parts A and B services are above or below the updated benchmark determined under § 425.601, § 425.602 or § 425.603. In order to qualify for a shared savings payment under the ENHANCED track, or to be responsible for sharing losses with CMS, an ACO's average per capita Medicare expenditures under the ACO for Medicare fee-for-service beneficiaries for Parts A and B services for the performance year must be below or above the updated benchmark, respectively, by at least the minimum savings or loss rate under paragraph (b) of this section.
(1) Risk adjustment for ACOs in agreement periods beginning on or before January 1, 2019. CMS does the following to adjust the benchmark each performance year:
(i) Newly assigned beneficiaries. CMS uses an ACO's prospective HCC risk score to adjust the benchmark for changes in severity and case mix in this population.
(ii) Continuously assigned beneficiaries.
(A) CMS uses demographic factors to adjust the benchmark for changes in the continuously assigned beneficiary population.
(B) If the prospective HCC risk score is lower in the performance year for this population, CMS adjusts the benchmark for changes in severity and case mix for this population using this lower prospective HCC risk score.
(2) Risk adjustment for ACOs in agreement periods beginning on July 1, 2019, and in subsequent years. CMS uses an ACO's prospective HCC risk score to adjust the benchmark for changes in severity and case mix in the assigned beneficiary population between BY3 and the performance year.
(i) Positive adjustments in prospective HCC risk scores are subject to a cap of 3 percent.
(ii) This cap is the maximum increase in risk scores for each agreement period, such that any positive adjustment between BY3 and any performance year in the agreement period cannot be larger than 3 percent.
(3) In risk adjusting the benchmark as described in §§ 425.601(a)(10), 425.602(a)(9) and 425.603(c)(10), CMS makes separate adjustments for each of the following populations of beneficiaries:
(i) ESRD.
(ii) Disabled.
(iii) Aged/dual eligible Medicare and Medicaid beneficiaries.
(iv) Aged/non-dual eligible Medicare and Medicaid beneficiaries.
(4)
(i) For performance years before 2017 to minimize variation from catastrophically large claims, CMS truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures as determined for each performance year.
(ii) For the 2017 performance year and subsequent performance years, to minimize variation from catastrophically large claims, CMS truncates an assigned beneficiary's total annual Parts A and B fee-for-service per capita expenditures at the 99th percentile of national Medicare fee-for-service expenditures as determined for the applicable performance year for assignable beneficiaries identified for the 12-month calendar year corresponding to the performance year.
(5) CMS uses a 3-month claims run out with a completion factor to calculate an ACO's per capita expenditures for each performance year.
(6) Calculations of the ACO's expenditures will include the payment amounts included in Part A and B fee-for-service claims.
(i) These calculations will exclude indirect medical education (IME) and disproportionate share hospital (DSH) payments.
(ii) These calculations will take into consideration individually beneficiary identifiable payments made under a demonstration, pilot or time limited program.
(A) For performance years beginning before 2018, these calculations will take into consideration all individually beneficiary identifiable payments, including interim payments, made under a demonstration, pilot or time limited program.
(B) For performance year 2018 and subsequent performance years, these calculations will take into consideration individually beneficiary identifiable final payments made under a demonstration, pilot or time limited program.
(7) In order to qualify for a shared savings payment, the ACO's average per capita Medicare expenditures for the performance year must be below the applicable updated benchmark by at least the minimum savings rate established for the ACO under paragraph (b) of this section.
(b) Minimum savings or loss rate.
(1) As part of the ACO's application for, or renewal of, program participation, the ACO must choose from the following options for establishing the MSR/MLR for the duration of the agreement period:
(i) Zero percent MSR/MLR
(ii) Symmetrical MSR/MLR in a 0.5 percent increment between 0.5-2.0 percent.
(iii) Symmetrical MSR/MLR that varies, based on the number of beneficiaries assigned to the ACO under subpart E of this part. The MSR for an ACO under the ENHANCED track is the same as the MSR that would apply in the one-sided model under either § 425.604(b) (for ACOs entering an agreement period on or before January 1, 2019) or § 425.605(b)(1) (for ACOs entering an agreement period on July 1, 2019, and in subsequent years) and is based on the number of assigned beneficiaries. The MLR under the ENHANCED track is equal to the negative MSR.
(2) To qualify for shared savings under the ENHANCED track, an ACO's average per capita Medicare expenditures for the performance year must be below its updated benchmark costs for the year by at least the MSR established for the ACO.
(3) To be responsible for sharing losses with the Medicare program, an ACO's average per capita Medicare expenditures for the performance year must be above its updated benchmark costs for the year by at least the MLR established for the ACO.
(c) Qualification for shared savings payment -
(1) For performance years (or a performance period) beginning on or before January 1, 2020. To qualify for shared savings, an ACO must meet the minimum savings rate requirement established under paragraph (b) of this section, meet the minimum quality performance standards established under § 425.502, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(2) For performance years beginning on or after January 1, 2021. To qualify for shared savings, an ACO must meet the minimum savings rate requirement established under paragraph (b) of this section, meet the quality performance standard established under § 425.512, and otherwise maintain its eligibility to participate in the Shared Savings Program under this part.
(d) Final sharing rate -
(1) For performance years (or a performance period) beginning on or before January 1, 2020. An ACO that meets all the requirements for receiving shared savings payments under the ENHANCED track will receive a shared savings payment of up to 75 percent of all the savings under the updated benchmark, as determined on the basis of its quality performance under § 425.502 (up to the performance payment limit described in paragraph (e)(2) of this section).
(2) For performance years beginning on or after January 1, 2021. An ACO that meets all the requirements for receiving shared savings payments under the ENHANCED track will receive a shared savings payment of 75 percent of all the savings under the updated benchmark (up to the performance payment limit described in paragraph (e)(2) of this section).
(e) Performance payment.
(1) If an ACO qualifies for savings by meeting or exceeding the MSR, the final sharing rate will apply to an ACO's savings on a first dollar basis.
(2) The amount of shared savings an eligible ACO receives under the ENHANCED track may not exceed 20 percent of its updated benchmark.
(f) Shared loss rate -
(1) For performance years (or a performance period) beginning on or before January 1, 2020. For an ACO that is required to share losses with the Medicare program for expenditures over the updated benchmark, the amount of shared losses is determined based on the inverse of its final sharing rate described in paragraph (d)(1) of this section (that is, 1 minus the final shared savings rate determined under paragraph (d)(1) of this section). The shared loss rate -
(i) May not exceed 75 percent; and
(ii) May not be less than 40 percent.
(2) For performance years beginning on or after January 1, 2021. For an ACO that is required to share losses with the Medicare program for expenditures over the updated benchmark, the amount of shared losses is determined as follows:
(i) If the ACO meets the quality performance standard established in § 425.512, CMS determines the shared loss rate as follows:
(A) Calculate the quotient of the MIPS Quality performance category points earned divided by the total MIPS Quality performance category points available.
(B) Calculate the product of the quotient determined in paragraph (f)(2)(i)(A) of this section, and 75 percent.
(C) Calculate the shared loss rate as 1 minus the product determined in paragraph (f)(2)(i)(B) of this section. The shared loss rate -
(1) May not exceed 75 percent; and
(2) May not be less than 40 percent.
(ii) If the ACO fails to meet the quality performance standard established in § 425.512, the shared loss rate is 75 percent.
(g) Loss recoupment limit. The amount of shared losses for which an eligible ACO is liable may not exceed 15 percent of its updated benchmark as determined under § 425.601, § 425.602 or § 425.603.
(h) Notification of savings and losses.
(1) CMS notifies an ACO in writing regarding whether the ACO qualifies for a shared savings payment, and if so, the amount of the payment due.
(2) CMS provides written notification to an ACO of the amount of shared losses, if any, that it must repay to the program.
(3) If an ACO has shared losses, the ACO must make payment in full to CMS within 90 days of receipt of notification.
(i) Extreme and uncontrollable circumstances. For performance year 2017 and subsequent performance years, the following adjustment is made in calculating the amount of shared losses, after the application of the shared loss rate in paragraph (f) of this section and the loss recoupment limit in paragraph (g) of this section.
(1) CMS determines the percentage of the ACO's performance year assigned beneficiary population affected by an extreme and uncontrollable circumstance.
(2) CMS reduces the amount of the ACO's shared losses by an amount determined by multiplying the shared losses by the percentage of the total months in the performance year affected by an extreme and uncontrollable circumstance, and the percentage of the ACO's assigned beneficiaries who reside in an area affected by an extreme and uncontrollable circumstance.
(i) For an ACO that is liable for a pro-rated share of losses under § 425.221(b)(2)(ii) or (b)(3)(i), the amount of shared losses determined for the performance year during which the termination becomes effective is adjusted according to this paragraph (i)(2).
(ii) [Reserved]
(3) CMS applies determinations made under the Quality Payment Program with respect to -
(i) Whether an extreme and uncontrollable circumstance has occurred; and
(ii) The affected areas.
(4) CMS has sole discretion to determine the time period during which an extreme and uncontrollable circumstance occurred and the percentage of the ACO's assigned beneficiaries residing in the affected areas.
(j) January 1, 2019 through June 30, 2019 performance year. Shared savings or shared losses for the January 1, 2019 through June 30, 2019 performance year are calculated as described in § 425.609.
(k) July 1, 2019 through December 31, 2019 performance year. Shared savings or shared losses for the July 1, 2019 through December 31, 2019 performance year are calculated as described in § 425.609.
[80 FR 32842, June 9, 2015, as amended at 81 FR 38017, June 10, 2016; 82 FR 53370, Nov. 15, 2017; 82 FR 60918, Dec. 26, 2017; 83 FR 60096, Nov. 23, 2018; 83 FR 68079, Dec. 31, 2018; 85 FR 85044, Dec. 28, 2020]
§ 425.611 Adjustments to Shared Savings Program calculations to address the COVID-19 pandemic.
(a) General. This section describes adjustments CMS makes to Shared Savings Program calculations to address the impact of the COVID-19 pandemic.
(b) Episodes of care for treatment of COVID-19.
(1) CMS identifies an episode of care for treatment of COVID-19 based on either of the following:
(i) Discharges for inpatient services eligible for the 20 percent adjustment under section 1886(d)(4)(C) of the Act.
(ii) Discharges for acute care inpatient services for treatment of COVID-19 from facilities that are not paid under the inpatient prospective payment system, such as CAHs, when the date of discharge occurs within the Public Health Emergency as defined in § 400.200 of this chapter.
(2) CMS defines the episode of care as starting in the month in which the inpatient stay begins as identified by the admission date, all months during the inpatient stay, and the month following the end of the inpatient stay as indicated by the discharge date.
(c) Applicability of adjustments. Notwithstanding any other provision in this part, CMS adjusts the following Shared Savings Program calculations to exclude all Parts A and B fee-for-service payment amounts for a beneficiary's episode of care for treatment of COVID-19 as described in paragraph (b) of this section:
(1) Calculation of Medicare Parts A and B fee-for-service expenditures for an ACO's assigned beneficiaries for all purposes including the following: Establishing, adjusting, updating, and resetting the ACO's historical benchmark and determining performance year expenditures.
(2) Calculation of fee-for-service expenditures for assignable beneficiaries as used in determining county-level fee-for-service expenditures and national Medicare fee-for-service expenditures, including the following calculations:
(i) Determining average county fee-for-service expenditures based on expenditures for the assignable population of beneficiaries in each county in the ACO's regional service area according to §§ 425.601(c) and 425.603(e) for purposes of calculating the ACO's regional fee-for-service expenditures.
(ii) Determining the 99th percentile of national Medicare fee-for-service expenditures for assignable beneficiaries for purposes of the following:
(A) Truncating assigned beneficiary expenditures used in calculating benchmark expenditures under §§ 425.601(a)(4), 425.602(a)(4), and 425.603(c)(4), and performance year expenditures under §§ 425.604(a)(4), 425.605(a)(3), 425.606(a)(4), and 425.610(a)(4).
(B) Truncating expenditures for assignable beneficiaries in each county for purposes of determining county fee-for-service expenditures according to §§ 425.601(c)(3) and 425.603(e)(3).
(iii) Determining 5 percent of national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program for assignable beneficiaries for purposes of capping the regional adjustment to the ACO's historical benchmark according to § 425.601(a)(8)(ii)(C).
(iv) Determining the flat dollar equivalent of the projected absolute amount of growth in national per capita expenditures for Parts A and B services under the original Medicare fee-for-service program for assignable beneficiaries, for purposes of updating the ACO's historical benchmark according to § 425.602(b)(2).
(v) Determining national growth rates that are used as part of the blended growth rates used to trend forward BY1 and BY2 expenditures to BY3 according to § 425.601(a)(5)(ii) and as part of the blended growth rates used to trend the benchmark and update the benchmark according to § 425.601(b)(2).
(3) Calculation of Medicare Parts A and B fee-for-service revenue of ACO participants for purposes of calculating the ACO's loss recoupment limit under the BASIC track as specified in § 425.605(d).
(4) Calculation of total Medicare Parts A and B fee-for-service revenue of ACO participants and total Medicare Parts A and B fee-for-service expenditures for the ACO's assigned beneficiaries for purposes of identifying whether an ACO is a high revenue ACO or low revenue ACO, as defined under § 425.20, and determining an ACO's eligibility for participation options according to § 425.600(d).
(5) Calculation or recalculation of the amount of the ACO's repayment mechanism arrangement according to § 425.204(f)(4).
[85 FR 27625, May 8, 2020, as amended at 85 FR 85044, Dec. 28, 2020]
§ 425.612 Waivers of payment rules or other Medicare requirements.
(a) General. CMS may waive certain payment rules or other Medicare requirements as determined necessary to carry out the Shared Savings Program under this part.
(1) SNF 3-day rule. For performance year 2017 and subsequent performance years, CMS waives the requirement in section 1861(i) of the Act for a 3-day inpatient hospital stay prior to a Medicare-covered post-hospital extended care service for eligible beneficiaries assigned to ACOs participating in a two-sided model and as provided in paragraph (a)(1)(iv) of this section during a grace period for beneficiaries excluded from prospective assignment to an ACO in a two-sided model, who receive otherwise covered post-hospital extended care services furnished by an eligible SNF that has entered into a written agreement to partner with the ACO for purposes of this waiver. Eligible SNFs include providers furnishing SNF services under swing bed agreements. All other provisions of the statute and regulations regarding Medicare Part A post-hospital extended care services continue to apply. ACOs identified under paragraph (a)(1)(vi) of this section may request to use the SNF 3-day rule waiver for performance years beginning on July 1, 2019, and in subsequent years.
(i) ACOs must submit to CMS supplemental application information sufficient to demonstrate the ACO has the capacity to identify and manage beneficiaries who would be either directly admitted to a SNF or admitted to a SNF after an inpatient hospitalization of fewer than 3-days in the form and manner specified by CMS. Application materials include but are not limited to, the following:
(A) Narratives describing how the ACO plans to implement the waiver. Narratives must include the following:
(1) The communication plan between the ACO and its SNF affiliates.
(2) A care management plan for beneficiaries admitted to a SNF affiliate.
(3) A beneficiary evaluation and admission plan approved by the ACO medical director and the healthcare professional responsible for the ACO's quality improvement and assurance processes under § 425.112.
(B) A list of SNFs with whom the ACO will partner along with executed written SNF affiliate agreements between the ACO and each listed SNF.
(ii) In order to be eligible to receive covered SNF services under the waiver, a beneficiary must meet the following requirements:
(A) In the case of a beneficiary who is assigned to an ACO that has selected preliminary prospective assignment with retrospective reconciliation under § 425.400(a)(2), the beneficiary must appear on the list of preliminarily prospectively assigned beneficiaries at the beginning of the performance year or on the first, second, or third quarterly preliminary prospective assignment list for the performance year in which they are admitted to the eligible SNF, and the SNF services must be provided after the beneficiary first appeared on the preliminary prospective assignment list for the performance year.
(B) In the case of a beneficiary who is assigned to an ACO that has selected prospective assignment under § 425.400(a)(3), the beneficiary must be prospectively assigned to the ACO for the performance year in which they are admitted to the eligible SNF.
(C) Does not reside in a SNF or other long-term care setting.
(D) Is medically stable.
(E) Does not require inpatient or further inpatient hospital evaluation or treatment.
(F) Have certain and confirmed diagnoses.
(G) Have an identified skilled nursing or rehabilitation need that cannot be provided as an outpatient.
(H) Have been evaluated and approved for admission to the SNF within 3 days prior to the SNF admission by an ACO provider/supplier who is a physician, consistent with the ACO's beneficiary evaluation and admission plan.
(iii) SNFs eligible to partner and enter into written agreements with ACOs for purposes of this waiver must do the following:
(A) Providers eligible to be included in the CMS 5-star Quality Rating System must have and maintain an overall rating of 3 or higher.
(B) Sign a SNF affiliate agreement with the ACO that includes elements determined by CMS including but not limited to the following:
(1) Agreement to comply with the requirements and conditions of this part, including but not limited to those specified in the participation agreement with CMS.
(2) Effective dates of the SNF affiliate agreement.
(3) Agreement to implement and comply with the ACO's beneficiary evaluation and admission plan and the care management plan.
(4) Agreement to validate the eligibility of a beneficiary to receive covered SNF services in accordance with the waiver prior to admission.
(5) Remedial processes and penalties that will apply for non-compliance.
(iv) For a beneficiary who was included on the ACO's prospective assignment list or preliminary prospective assignment list at the beginning of the performance year or on the first, second, or third quarterly preliminary prospective assignment list for the performance year, for an ACO for which a waiver of the SNF 3-day rule has been approved under paragraph (a)(1) of this section, but who was subsequently removed from the assignment list for the performance year, CMS makes payment for SNF services furnished to the beneficiary by a SNF affiliate if the following conditions are met:
(A)
(1) The beneficiary was prospectively assigned to an ACO that selected prospective assignment under § 425.400(a)(3) at the beginning of the applicable performance year, but was excluded in the most recent quarterly update to the assignment list under § 425.401(b), and the beneficiary was admitted to a SNF affiliate within 90 days following the date that CMS delivered the quarterly exclusion list to the ACO; or
(2) The beneficiary was identified as preliminarily prospectively assigned to an ACO that has selected preliminary prospective assignment with retrospective reconciliation under § 425.400(a)(2) in the report provided under § 425.702(c)(1)(ii)(A) at the beginning of the performance year or for the first, second, or third quarter of the performance year, the SNF services were provided after the beneficiary first appeared on the preliminary prospective assignment list for the performance year, and the beneficiary meets the criteria to be assigned to an ACO under § 425.401(a)(1) and (2).
(B) But for the beneficiary's removal from the ACO's assignment list, CMS would have made payment to the SNF affiliate for such services under the waiver under paragraph (a)(1) of this section.
(v) The following beneficiary protections apply when a beneficiary receives SNF services without a prior 3-day inpatient hospital stay from a SNF affiliate that intended to provide services under a SNF 3-day rule waiver under paragraph (a)(1) of this section, the SNF affiliate services were non-covered only because the SNF affiliate stay was not preceded by a qualifying hospital stay under section 1861(i) of the Act, and in the case of a beneficiary where the ACO selected one of the following:
(A) Prospective assignment under § 425.400(a)(3), the beneficiary was not prospectively assigned to the ACO for the performance year in which they received the SNF services, or was prospectively assigned but was later excluded and the 90-day grace period, described in paragraph (a)(1)(iv)(A) of this section, has lapsed.
(B) Preliminary prospective assignment with retrospective reconciliation under § 425.400(a)(2), the beneficiary was not identified as preliminarily prospectively assigned to the ACO for the performance year in the report provided under § 425.702(c)(1)(ii)(A) at the beginning of the performance year or for the first, second, or third quarter of the performance year before the SNF services were provided to the beneficiary.
(C) A SNF is presumed to intend to provide services pursuant to the SNF 3-day rule waiver under paragraph (a)(1) of this section if the SNF submitting the claim is a SNF affiliate of an ACO for which such a waiver has been approved.
(D) CMS makes no payments for SNF services to a SNF affiliate of an ACO for which a waiver of the SNF 3-day rule has been approved when the SNF affiliate admits a FFS beneficiary who was not prospectively or preliminarily prospectively assigned to the ACO prior to the SNF admission or was prospectively assigned but was later excluded and the 90-day grace period under paragraph (a)(1)(iv)(A) of this section has lapsed.
(E) In the event that CMS makes no payment for SNF services furnished by a SNF affiliate as a result of paragraph (a)(1)(v)(D) of this section and the only reason the claim was non-covered is due to the lack of a qualifying inpatient stay, the following beneficiary protections will apply:
(1) The SNF must not charge the beneficiary for the expenses incurred for such services; and
(2) The SNF must return to the beneficiary any monies collected for such services; and
(3) The ACO may be required to submit a corrective action plan under § 425.216(b) for CMS approval. If after being given an opportunity to act upon the corrective action plan the ACO fails to come into compliance with the requirements of paragraph (a)(1), approval for the SNF 3-day rule waiver under this section will be terminated as provided under paragraph (d) of this section.
(2) [Reserved]
(b) Review and determination of request to use waivers.
(1) In order to obtain a determination regarding whether the ACO may use waivers under this section, an ACO must submit a waiver request to CMS in the form and manner and by a deadline specified by CMS.
(2) An ACO executive who has the authority to legally bind the ACO must certify to the best of his or her knowledge, information, and belief that the information contained in the waiver request submitted under paragraph (b)(1) of this section is accurate, complete, and truthful.
(3) CMS evaluates an ACO's waiver request to determine whether it satisfies the requirements of this part and approves or denies waiver requests accordingly. Waiver requests are approved or denied on the basis of the following:
(i) Information contained in and submitted with the waiver request by a deadline specified by CMS.
(ii) Supplemental information submitted by a deadline specified by CMS in response to a CMS request for information.
(iii) Screening of the ACO, ACO participants, ACO providers/suppliers, and other individuals or entities providing services to Medicare beneficiaries in accordance with the terms of the waiver.
(iv) Other information available to CMS.
(4) CMS may deny a waiver request if an ACO fails to submit requested information by the deadlines established by CMS.
(c) Effective and termination date of waivers.
(1) Waivers are effective upon CMS notification of approval for the waiver or the start date of the participation agreement, whichever is later.
(2) Waivers do not extend beyond the end of the participation agreement.
(3) If CMS terminates the participation agreement under § 425.218, the waiver ends on the date specified by CMS in the termination notice.
(4) If the ACO terminates the participation agreement, the waiver ends on the effective date of termination as specified in the written notification required under § 425.220.
(d) Monitoring and termination of waivers.
(1) ACOs with approved waivers are required to post their use of the waiver as part of public reporting under § 425.308.
(2) CMS monitors and audits the use of such waivers in accordance with § 425.316.
(3) CMS reserves the right to deny or revoke a waiver if an ACO, its ACO participants, ACO providers/suppliers or other individuals or entities providing services to Medicare beneficiaries are not in compliance with the requirements of this part or if any of the following occur:
(i) The waiver is not used as described in the ACO's waiver request under paragraph (b)(1) of this section.
(ii) The ACO does not successfully meet the quality reporting standard under subpart F of this part.
(iii) CMS identifies a program integrity issue affecting the ACO's use of the waiver.
(4) CMS reserves the right to take compliance action, including termination, against an ACO for noncompliance with program rules, including misuse of a waiver under this section, as specified at §§ 425.216 and 425.218.
(e) Other rules governing use of waivers.
(1) Waivers under this section do not protect financial or other arrangements between or among ACOs, ACO participants, ACO providers/suppliers, or other individual or entities providing services to Medicare beneficiaries from liability under the fraud and abuse laws or any other applicable laws.
(2) Waivers under this section do not protect any person or entity from liability for any violation of law or regulation for any conduct other than the conduct permitted by a waiver under paragraph (a) of this section.
(3) ACOs must ensure compliance with all claims submission requirements, except those expressly waived under paragraph (a) of this section.
(f) Waiver for payment for telehealth services. For performance year 2020 and subsequent performance years, CMS waives the originating site requirements in section 1834(m)(4)(C)(i) and (ii) of the Act and makes payment for telehealth services furnished to a beneficiary, if the following conditions are met:
(1) The beneficiary was prospectively assigned to an ACO that is an applicable ACO for purposes of § 425.613 at the beginning of the applicable performance year, but the beneficiary was excluded in the most recent quarterly update to the prospective assignment list under § 425.401(b).
(2) The telehealth services are provided by a physician or practitioner billing under the TIN of an ACO participant in the ACO within 90 days following the date CMS delivers the quarterly exclusion list to the ACO.
(3) But for the beneficiary's exclusion from the ACO's prospective assignment list, CMS would have made payment to the ACO participant for such services under § 425.613.
[80 FR 32843, June 9, 2015, as amended at 81 FR 80561, Nov. 15, 2016; 82 FR 53371, Nov. 15, 2017; 83 FR 68080, Dec. 31, 2018; 84 FR 63204, Nov. 15, 2019]
§ 425.613 Telehealth services.
(a) General. Payment is available for otherwise covered telehealth services furnished on or after January 1, 2020, by a physician or other practitioner billing through the TIN of an ACO participant in an applicable ACO, without regard to the geographic requirements under section 1834(m)(4)(C)(i) of the Act, in accordance with the requirements of this section.
(1) For purposes of this section:
(i) An applicable ACO is an ACO that is participating under a two-sided model under § 425.600 and has elected prospective assignment under § 425.400(a)(3) for the performance year.
(ii) The home of the beneficiary is treated as an originating site under section 1834(m)(4)(C)(ii) of the Act.
(2) For payment to be made under this section, the following requirements must be met:
(i) The beneficiary is prospectively assigned to the ACO for the performance year in which the beneficiary received the telehealth service.
(ii) The physician or practitioner who furnishes the telehealth service must bill under the TIN of an ACO participant that is included on the certified ACO participant list under § 425.118 for the performance year in which the service is rendered.
(iii) The originating site must comply with applicable State licensing requirements.
(iv) When the originating site is the beneficiary's home, the telehealth services must not be inappropriate to furnish in the home setting. Services that are typically furnished in an inpatient setting may not be furnished as a telehealth service when the originating site is the beneficiary's home.
(v) CMS does not pay a facility fee when the originating site is the beneficiary's home.
(b) Beneficiary protections.
(1) When a beneficiary who is not prospectively assigned to an applicable ACO or in a 90-day grace period under § 425.612(f) receives a telehealth service from a physician or practitioner billing through the TIN of an ACO participant participating in an applicable ACO, CMS makes no payment for the telehealth service to the ACO participant.
(2) In the event that CMS makes no payment for a telehealth service furnished by a physician or practitioner billing through the TIN of an ACO participant, and the only reason the claim was non-covered is because the beneficiary is not prospectively assigned to the ACO or in the 90-day grace period under § 425.612(f), all of the following beneficiary protections apply:
(i) The ACO participant must not charge the beneficiary for the expenses incurred for such service.
(ii) The ACO participant must return to the beneficiary any monies collected for such service.
(iii) The ACO may be required to submit a corrective action plan under § 425.216(b) for CMS approval. If the ACO is required to submit a corrective action plan and, after being given an opportunity to act upon the corrective action plan, the ACO fails to implement the corrective action plan or demonstrate improved performance upon completion of the corrective action plan, CMS may terminate the participation agreement as specified under § 425.216(b)(2).
(c) Termination date for purposes of payment for telehealth services.
(1) Payment for telehealth services under paragraph (a) of this section does not extend beyond the end of the applicable ACO's participation agreement.
(2) If CMS terminates the participation agreement under § 425.218, payment for telehealth services under paragraph (a) of this section is not made with respect to telehealth services furnished beginning on the date specified by CMS in the termination notice.
(3) If the ACO terminates the participation agreement, payment for telehealth services under paragraph (a) of this section is not made with respect to telehealth services furnished beginning on the effective date of termination as specified in the written notification required under § 425.220.
(d) Monitoring of telehealth services.
(1) CMS monitors and audits the use of telehealth services by the ACO and its ACO participants and ACO providers/suppliers, in accordance with § 425.316.
(2) CMS reserves the right to take compliance action, up to and including termination of the participation agreement, as specified in §§ 425.216 and 425.218, with respect to an applicable ACO for non-compliance with program requirements, including inappropriate use of telehealth services.
[83 FR 68081, Dec. 31, 2018]
Subpart H - Data Sharing With ACOs
§ 425.700 General rules.
(a) CMS shares aggregate reports with the ACO.
(b) CMS shares beneficiary identifiable data with ACOs on the condition that the ACO, its ACO participants, ACO providers/suppliers, and other individuals or entities performing functions or services related to the ACO's activities observe all relevant statutory and regulatory provisions regarding the appropriate use of data and the confidentiality and privacy of individually identifiable health information and comply with the terms of the data use agreement described in this subpart.
(c) The ACO must not limit or restrict appropriate sharing of medical record data with providers and suppliers both within and outside the ACO in accordance with applicable law.
§ 425.702 Aggregate reports.
CMS shares aggregate reports with ACOs as follows:
(a) Aggregate reports are shared at the start of the agreement period based on beneficiary claims data used to calculate the benchmark, and each quarter thereafter during the agreement period.
(b) These aggregate reports include, when available, the following information, deidentified in accordance with 45 CFR 164.514(b):
(1) Aggregated metrics on the assigned beneficiary population.
(2) Utilization and expenditure data at the start of the agreement period based on historical beneficiaries used to calculate the benchmark.
(c)
(1)
(i) For performance years 2012 through 2015, at the beginning of the agreement period, during each quarter (and in conjunction with the annual reconciliation), and at the beginning of each performance year, CMS, upon the ACO's request for the data for purposes of population-based activities relating to improving health or reducing growth in health care costs, process development, case management, and care coordination, will provide the ACO with information regarding preliminarily prospectively assigned beneficiaries whose data was used to generate the aggregate data reports under paragraphs (a) and (b) of this section. The information includes the following:
(A) Beneficiary name.
(B) Date of birth.
(C) HICN.
(D) Sex.
(ii) For performance year 2016 and subsequent performance years, at the beginning of the agreement period, during each quarter (and in conjunction with the annual reconciliation), and at the beginning of each performance year, CMS, upon the ACO's request for the data for purposes of population-based activities relating to improving health or reducing growth in health care costs, process development, case management, and care coordination, provides the ACO with information about its fee-for-service population.
(A) For an ACO participating under preliminary prospective assignment with retrospective reconciliation as specified under § 425.400(a)(2), the following information is made available regarding preliminarily prospectively assigned beneficiaries and beneficiaries that received a primary care service during the previous 12 months from one of the ACO participants that submits claims for primary care services used to determine the ACO's assigned population under subpart E of this part:
(1) Beneficiary name.
(2) Date of birth.
(3) Health Insurance Claim Number (HICN).
(4) Sex.
(B) For an ACO participating under preliminary prospective assignment with retrospective reconciliation as specified under § 425.400(a)(2), information in the following categories, which represents the minimum data necessary for ACOs to conduct health care operations work, is made available regarding preliminarily prospectively assigned beneficiaries:
(1) Demographic data such as enrollment status.
(2) Health status information such as risk profile and chronic condition subgroup.
(3) Utilization rates of Medicare services such as the use of evaluation and management, hospital, emergency, and post-acute services, including the dates and place of service.
(4) Expenditure information related to utilization of services.
(C) The information under paragraphs (c)(1)(ii)(A) and (B) of this section is made available to ACOs participating under prospective assignment as specified under § 425.400(a)(3), but is limited to the ACO's prospectively assigned beneficiaries.
(2) In its request for these data, the ACO must certify that it is seeking the following information:
(i) As a HIPAA-covered entity, and the request reflects the minimum data necessary for the ACO to conduct its own health care operations work that falls within the first or second paragraph of the definition of health care operations at 45 CFR 164.501.
(ii) As the business associate of its ACO participants and ACO providers/suppliers, who are HIPAA-covered entities, and the request reflects the minimum data necessary for the ACO to conduct health care operations work that falls within the first or second paragraph of the definition of health care operations at 45 CFR 164.501 on behalf of those participants.
(d) For an ACO eligible to be reconciled under § 425.609(b), CMS shares with the ACO quarterly aggregate reports as provided in paragraphs (b) and (c)(1)(ii) of this section for CY 2019.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32844, June 9, 2015; 83 FR 60096, Nov. 23, 2018; 83 FR 68081, Dec. 31, 2018]
§ 425.704 Beneficiary-identifiable claims data.
Subject to providing the beneficiary with the opportunity to decline data sharing as described in this § 425.708, and subject to having a valid DUA in place, CMS, upon the ACO's request for the data for purposes of evaluating the performance of its ACO participants or its ACO providers/suppliers, conducting quality assessment and improvement activities, and conducting population-based activities relating to improved health, will provide the ACO with beneficiary identifiable claims data for preliminarily prospectively and prospectively assigned beneficiaries and other beneficiaries who receive primary care services from an ACO participant that submits claims for primary care services used to determine the ACO's assigned population under subpart E of this part during the performance year.
(a) If an ACO wishes to receive beneficiary identifiable claims data, it must sign a DUA and it must submit a formal request for data. ACOs may access requested data as often as once per month.
(b) The ACO must certify that it is requesting claims data about either of the following:
(1) Its own patients, as a HIPAA-covered entity, and the request reflects the minimum data necessary for the ACO to conduct its own health care operations work that falls within the first or second paragraph of the definition of health care operations at 45 CFR 164.501.
(2) The patients of its HIPAA-covered entity ACO participants or its ACO providers/suppliers as the business associate of these HIPAA covered entities, and the request reflects the minimum data necessary for the ACO to conduct health care operations work that falls within the first or second paragraph of the definition of health care operations at 45 CFR 164.501 on behalf of those participants.
(c) The use of identifiers and claims data will be limited to developing processes and engaging in appropriate activities related to coordinating care and improving the quality and efficiency of care that are applied uniformly to all Medicare beneficiaries with primary care services at the ACO, and that these data will not be used to reduce, limit or restrict care for specific beneficiaries.
(d) To ensure that beneficiaries have a meaningful opportunity to decline having their claims data shared with the ACO, the ACO may only request claims data about a beneficiary if -
(1) For an ACO participating under -
(i) Preliminary prospective assignment with retrospective reconciliation as specified under § 425.400(a)(2), the beneficiary's name appears on the preliminary prospective assignment list provided to the ACO at the beginning of the performance year, during each quarter (and in conjunction with the annual reconciliation) or the beneficiary has received a primary care service from an ACO participant upon whom assignment is based (under subpart E of this part) during the most recent 12-month period; or
(ii) Prospective assignment as specified under § 425.400(a)(3), the beneficiary's name appears on the prospective assignment list provided to the ACO at the beginning of the performance year.
(2) The beneficiary has been notified in compliance with § 425.708 that the ACO has requested access to beneficiary identifiable claims data in order to improve the quality of care that is furnished to the beneficiary and, where applicable, coordinate care offered to the beneficiary; and
(3) The beneficiary did not exercise the opportunity to decline having his/her claims data shared with the ACO as provided in § 425.708.
(e) At the ACO's request, CMS continues to provide ACOs with updates to the requested beneficiary identifiable claims data, subject to beneficiary's opportunity to decline data sharing under § 425.708.
(f) If an ACO requests beneficiary identifiable information, compliance with the terms of the data use agreement described in § 425.710 is a condition of an ACO's participation in the Shared Savings Program.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32844, June 9, 2015; 83 FR 68082, Dec. 31, 2018]
§ 425.706 Minimum necessary data.
(a) ACOs must limit their identifiable data requests to the minimum necessary to accomplish a permitted use of the data. The minimum necessary Parts A and B data elements may include but are not limited to the following data elements:
(1) Beneficiary ID.
(2) Procedure code.
(3) Gender.
(4) Diagnosis code.
(5) Claim ID.
(6) The from and through dates of service.
(7) The provider or supplier ID.
(8) The claim payment type.
(9) Date of birth and death, if applicable.
(10) TIN.
(11) NPI.
(b) The minimum necessary Part D data elements may include but are not limited to the following data elements:
(1) Beneficiary ID.
(2) Prescriber ID.
(3) Drug service date.
(4) Drug product service ID.
(5) Quantity dispensed.
(6) Days supplied.
(7) Brand name.
(8) Generic name.
(9) Drug strength.
(10) TIN.
(11) NPI.
(12) Indication if on formulary.
(13) Gross drug cost.
§ 425.708 Beneficiaries may decline claims data sharing.
(a) Beneficiaries must receive notification about the Shared Savings Program and the opportunity to decline claims data sharing and instructions on how to inform CMS directly of their preference.
(1) FFS beneficiaries are notified about the opportunity to decline claims data sharing through CMS materials such as the Medicare & You Handbook and through the notifications required under § 425.312.
(2) The notifications provided under § 425.312 must state that the ACO may have requested beneficiary identifiable claims data about the beneficiary for purposes of its care coordination and quality improvement work, and inform the beneficiary how to decline having his or her claims information shared with the ACO in the form and manner specified by CMS.
(3) Beneficiary requests to decline claims data sharing will remain in effect unless and until a beneficiary subsequently contacts CMS to amend that request to permit claims data sharing with ACOs.
(b) The opportunity to decline having claims data shared with an ACO under paragraph (a) of this section does not apply to the information that CMS provides to ACOs under § 425.702(c).
(c) In accordance with 42 U.S.C. 290dd-2 and the implementing regulations at 42 CFR part 2, CMS does not share beneficiary identifiable claims data relating to the diagnosis and treatment of alcohol and substance abuse without the explicit written consent of the beneficiary.
(d) The provisions of this section relate only to the sharing of Medicare claims data between the Medicare program and the ACO under the Shared Savings Program and are in no way intended to impede existing or future data sharing under other authorities.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32840, June 9, 2015]
§ 425.710 Data use agreement.
(a)
(1) Before receiving any beneficiary identifiable data, ACOs must enter into a DUA with CMS. Under the DUA, the ACO must comply with the limitations on use and disclosure that are imposed by HIPAA, the applicable DUA, and the statutory and regulatory requirements of the Shared Savings Program.
(2) If the ACO misuses or discloses data in a manner that violates any applicable statutory or regulatory requirements or that is otherwise non-compliant with the provisions of the DUA, it will no longer be eligible to receive data under subpart H of this part, may be terminated from the Shared Savings Program under § 425.218, and may be subject to additional sanctions and penalties available under the law.
(b) [Reserved]
Subpart I - Reconsideration Review Process
§ 425.800 Preclusion of administrative and judicial review.
(a) There is no reconsideration, appeal, or other administrative or judicial review of the following determinations under this part:
(1) The specification of quality and performance standards under §§ 425.500, 425.502, 425.510, and 425.512.
(2) The assessment of the quality of care furnished by an ACO under the performance standards established in § 425.502 or § 425.512, as applicable.
(3) The assignment of Medicare fee-for-service beneficiaries under Subpart E of this part.
(4) The initial determination or revised initial determination of whether an ACO is eligible for shared savings, and the amount of such shared savings, including the initial determination or revised initial determination of the estimated average per capita Medicare expenditures under the ACO for Medicare fee-for-service beneficiaries assigned to the ACO and the average benchmark for the ACO in accordance with section 1899(d) of the Act, as implemented under §§ 425.601, 425.602, 425.603, 425.604, 425.605, 425.606, and 425.610.
(5) The percent of shared savings specified by the Secretary and the limit on the total amount of shared savings established under §§ 425.604, 425.605, 425.606, and 425.610.
(6) The termination of an ACO for failure to meet the quality performance standards established under § 425.502 or § 425.512, as applicable.
(7) The termination of a beneficiary incentive program established under § 425.304(c).
(b) [Reserved]
[76 FR 67973, Nov. 2, 2011, as amended at 81 FR 38017, June 10, 2016; 83 FR 68082, Dec. 31, 2018; 85 FR 85044, Dec. 28, 2020]
§ 425.802 Request for review.
(a) An ACO may appeal an initial determination that is not prohibited from administrative or judicial review under § 425.800 by requesting a reconsideration review by a CMS reconsideration official.
(1) An ACO that wants to request reconsideration review by a CMS reconsideration official must submit a written request by an authorized official for receipt by CMS within 15 days of the notice of the initial determination.
(i) If the 15th day is a weekend or a Federal holiday, then the timeframe is extended until the end of the next business day.
(ii) Failure to submit a request for reconsideration within 15 days will result in denial of the request for reconsideration.
(2) The reconsideration review must be held on the record (review of submitted documentation).
(b) An ACO that requests a reconsideration review for termination will remain operational throughout the review process.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32845, June 9, 2015]
§ 425.804 Reconsideration review process.
(a) Acknowledgement of reconsideration review request. The reconsideration official sends an acknowledgement of the reconsideration review request to the ACO and CMS that includes the following:
(1) Review procedures.
(2) Procedures for submission of evidence including format and timelines.
(3) A briefing schedule that permits each party to submit only one written brief, including any evidence, for consideration by the reconsideration official in support of the party's position. The submission of any additional briefs or supplemental evidence will be at the sole discretion of the reconsideration official.
(b) Burden of proof, standard of proof, and standards of review. The burden of proof is on the ACO to demonstrate to the reconsideration official with convincing evidence that the initial determination is not consistent with the requirements of this part or applicable statutory authority.
(c) Reconsideration official. The reconsideration official is an independent CMS official who did not participate in the initial determination that is being reviewed.
(d) Evidence.
(1) The reconsideration official's review will be based only on evidence submitted by the reconsideration official's requested deadline, unless otherwise requested by the reconsideration official.
(2) Documentation submitted for the record as evidence cannot be documentation that was not previously submitted to CMS by the applicable deadline and in the requested format.
(3) All evidence submitted by the ACO and CMS, in preparation for the reconsideration review will be shared with the other party to the hearing.
(e) The reconsideration official will notify CMS and the ACO of his or her recommendation.
[76 FR 67973, Nov. 2, 2011, as amended at 80 FR 32845, June 9, 2015]
§ 425.806 On-the-record review of reconsideration official's recommendation by independent CMS official.
(a)
(1) If CMS or the ACO disagrees with the recommendation of the reconsideration official, it may request an on the record review of the initial determination and recommendation by an independent CMS official who was not involved in the initial determination or the reconsideration review process.
(2) In order to request an on-the-record review, CMS or the ACO must submit an explanation of why it disagrees with the recommendation by the timeframe and in the format indicated in the reconsideration official's recommendation letter.
(b) The on-the-record review process is based only on evidence presented during the reconsideration review.
(c) The independent CMS official considers the recommendation of the reconsideration official and makes a final agency determination.
§ 425.808 Effect of independent CMS official's decision.
(a) The decision of the independent CMS official is final and binding.
(b) The reconsideration review process under this subpart must not be construed to negate, diminish, or otherwise alter the applicability of existing laws, rules, and regulations or determinations made by other government agencies.
§ 425.810 Effective date of decision.
(a) If the initial determination denying an ACO's application to participate in the Shared Savings Program is upheld, the application will remain denied based on the effective date of the original notice of denial.
(b) If the initial determination to terminate an agreement with an ACO is upheld, the decision to terminate the agreement is effective as of the date indicated in the initial notice of termination.
(c) If the initial determination to terminate an ACO is reversed, the ACO is reinstated into the Shared Savings Program, retroactively back to the original date of termination.